
I am an addict. Today is the day I have chosen not to be ruled any longer by the indulgences of temporary satisfaction. Too long has the grasping hands of drugs alcohol tobacco sex the pursuit of wealth and other evils held tight to thoughts impure. Man has become a race of insert drug hereheads.My own dealings have been in all of the above at one point or another. These are not necessaril
Dancing in the Streets
I have been told that the sun rests so we may sin in the night and start fresh again with a mulligan for a baptism in a new sun's rays washes the dirt from the heavy soul. My mulligan started like many others before with prospects of a new beginning and little or no rest from the playing out of how a night was going to go in my head. I never anticipated that the darkest night could end brighter
A Thousand Loves A Thousand Heartbreaks
The way of life that is the traveler is the most fulfilling and emptying existence one can know. He follows a strict Code of the Road that requires devout faith in wanderings toward the direction of dreams. It is a manual instructing on the dealings of the comedies and tragedies experienced during his pilgrimage as well as a moral support beam when struggling to remind oneself to keep afoot and
Being Negative Is Not So Bad
A new study published in PLOS Biology looks at the potential magnitude and effect of publication bias in animal trials. Essentially, the authors conclude that there is a significant file-drawer effect – failure to publish negative studies – with animal studies and this impacts the translation of animal research to human clinical trials.
SBM is greatly concerned with the technology of medical science. On one level, the methods of individual studies need to be closely analyzed for rigor and bias. But we also go to great pains to dispel the myth that individual studies can tell us much about the practice of medicine.
Reliable conclusions come from interpreting the literature as a whole, and not just individual studies. Further, the whole of the literature is greater than the sum of individual studies – there are patterns and effects in the literature itself that need to be considered.
One big effect is the file-drawer effect, or publication bias – the tendency to publish positive studies more than negative studies. A study showing that a treatment works or has potential is often seen as doing more for the reputation of a journal and the careers of the scientists than negative studies. So studies with no measurable effect tend to languish unpublished.
Individual studies looking at an ineffective treatment (if we assume perfect research methodology) should vary around no net effect. If those studies that are positive at random are more likely to be published than those studies that are neutral or negative, than any systematic review of the published literature is likely to find a falsely positive effect.
Of course, we do not live in a perfect world and many studies have imperfect methods and even hidden biases. So in reality there is likely to be a positive bias to the studies. This positive bias magnifies the positive publication bias.
There are attempts in the works to mitigate the problem of publication bias in the clinical literature. For example, clinicaltrials.gov is a registry of all trials involving human subjects – before the trials are completed and the results known. This way reviewers can have access to all the data – not just the data researchers and journal editors deem worthy.
This new study seeks to explore if publication bias is similarly a problem with animal studies. The issues are similar to human trials. There is an ethical question, as sacrificing animals in research is justified by the data we get in return. If that data is hidden and does not become part of the published record, than the animals were sacrificed for nothing.
And also, publication bias can lead to false conclusions. This in turn can, for example, lead to clinical trials of a drug that seems promising in animal studies. This could potentially expose human subjects to a harmful or just worthless drug that would not have made it to human trials if all the negative animal data were published.
The study itself looked at a database of animal models of stroke. They examined 525 publications involving 16 different stroke interventions. There are a few different types of statistical analysis that can be done to infer probable publication bias. Basically, without publication bias there should be a certain distribution of findings in terms of effect sizes. If only positive or larger effect sizes are being published, then the distribution will be skewed.
This type of analysis provides an estimation only. They found that:
Egger regression and trim-and-fill analysis suggested that publication bias was highly prevalent (present in the literature for 16 and ten interventions, respectively) in animal studies modelling stroke. Trim-and-fill analysis suggested that publication bias might account for around one-third of the efficacy reported in systematic reviews, with reported efficacy falling from 31.3% to 23.8% after adjustment for publication bias. We estimate that a further 214 experiments (in addition to the 1,359 identified through rigorous systematic review; non publication rate 14%) have been conducted but not reported. It is probable that publication bias has an important impact in other animal disease models, and more broadly in the life sciences.
So there was some disagreement between the methods used, but both showed that there is likely to be a significant publication bias. If their analysis is correct, about one third of systematic reviews of animal studies in stroke that conclude an intervention works may be due to publication bias rather than a real effect. The authors also speculate that this effect is likely not unique to stroke, and may be generalizable to animal studies in general.
Of course, this is just an individual study, and further analysis using different data sets are needed to confirm these results.
Conclusion
The results of this study are not surprising and are in line with what is known from examining clinical trials. They suggest that similar methods to minimize publication bias are necessary for animal studies in addition to human trials.
Hopefully, this kind of self-critical analysis will lead to improvement in the technology of medical research. It should further lead to more caution in interpreting not only single studies but systematic reviews.
Also, in my opinion, it highlights the need to consider basic science and plausibility in evaluating animal and clinical trials.
![]()
SBM Live Event – April 17th
A panels of bloggers from SBM will be taking part in the Northeast Conference on Science and Skepticism – NECSS 2010, April 17th beginning 10:00AM in New York.
There will be a 70 minute panel discussion moderated by John Snyder and featuring David Gorski, Kimball Atwood, Val Jones, and myself – Steven Novella. The topic of discussion will be the infiltration of pseudoscience into academic medicine.
This will be part of a full day of science featuring other excellent speakers, including James Randi, D. J. Grothe, Steve Mirsky, George Hrab, and Julia Galef. There will also be a live recording of the wildly popular science podcast, The Skeptics’ Guide to the Universe.
Go to http://www.NECSScon.org to register.
![]()
Genetic Testing for Patients on Coumadin
Anticoagulation is advised for patients who have had a blood clot or who are at increased risk of blood clots because of atrial fibrillation, artificial heart valves, or other conditions. Over 30 million prescriptions are written every year in the US for the anticoagulant warfarin, best known under the brand name Coumadin. Originally developed as a rat poison, warfarin has proved very effective in preventing blood clots and saving lives; but too much anticoagulation leads to the opposite problem: bleeding. A high level of Coumadin might prevent a stroke from a blood clot only to cause a stroke from an intracranial bleed. The effect varies from person to person and from day to day depending on things like the amount of vitamin K in the diet and interactions with other medications. It requires careful monitoring with blood tests, and it is tricky because there is a delay between changing the dose and seeing the results.
In his book The Language of Life, Francis Collins predicts that Coumadin will be the first drug for which the so-called Dx-Rx paradigm — a genetic test (Dx) followed by a prescription (Rx) — will enter mainstream medical practice. FDA economists have estimated that by formally integrating genetic testing into routine warfarin therapy, the US alone would avoid 85,000 serious bleeding events and 17,000 strokes annually.
A recent news release from the American College of Cardiology described a paper at their annual meeting reporting a study of
896 people who, shortly after beginning warfarin therapy, gave a blood sample or cheek swab that was analyzed for expression of two genes — CYP2C9 and VKORC1 — that revealed sensitivity to warfarin. People with high sensitivity were put on a reduced dose of warfarin and had frequent blood tests. People with low sensitivity were given a higher dose of warfarin.
During the first six months that they took warfarin, those who underwent genetic testing were 31 percent less likely to be hospitalized for any reason and 29 percent less likely to be hospitalized for bleeding or thromboembolism than were a group that did not have genetic testing.
Epstein said that the cost of the genetic testing — $250 to $400 — would be justified by reduced hospitalization costs.
At this point, I don’t believe this study. I’ll explain why I’m skeptical.
It seems to me something is wrong with the whole idea of using genetic testing to adjust Coumadin dosage. It doesn’t matter whether a patient has low sensitivity or high sensitivity to warfarin, since the same trial-and-error process of monitoring and dose adjustment will result in a safe dose for either.
In the typical scenario for a patient who is given warfarin, he is in the hospital where he is first given heparin by injection, usually in the form of low molecular weight heparins like Lovenox. Heparin works by binding to antithrombin and does not require monitoring with blood tests. Warfarin works by an entirely different mechanism. It reduces the amount of vitamin K dependent clotting factors. The heparin provides immediate protection while the warfarin gradually takes effect, a process that lasts for several days and lags behind the blood test used to monitor it: prothrombin time with calculation of the International Normalized Ratio (INR). After the INR reaches the target levels (usually 2-3 times normal), the injectable drug is stopped.
Apparently some providers are in a hurry to get the patient stabilized on Coumadin, so they start with a high “loading” dose and then back off as needed. This may have made sense when patients had to be off the heparin before they could be discharged from the hospital; but today they are commonly taught to give themselves subcutaneous injections and they are sent home, continuing the Lovenox until the Coumadin kicks in. There’s no reason they couldn’t start everyone on a low dose of Coumadin and adjust upwards as needed. Blood tests are done very frequently at first (as often as every day or two) and then can be cut back to as infrequently as once a month if the INR remains stable on a constant dose of warfarin. In the medical facility where I get my care, a Coumadin Clinic directed by a clinical pharmacologist monitors all patients on Coumadin.
A start low/adjust upwards protocol will result in a safe dose for all patients regardless of their DNA. I don’t see how that management plan would be improved by knowing the gene expressions. It takes time to get the genetic test results, and the provider has to start the patient on Coumadin before the test results are even available. Genetics is only estimated to contribute about 70% to dose requirements, and variations in the other 30% could outweigh simplistic dose estimates based on DNA. And testing costs money that I see no need to spend.
It will be interesting to read the actual study when it is published. I will be looking closely for confounding factors that might have influenced results. Could the tested patients have been treated differently in some way because of expectations raised by the DNA test? Did the non-tested patients have optimal management by someone experienced in adjusting Coumadin dosage? Was the study population somehow different from the population the average doctor sees in his practice? How exactly was the Coumadin dose adjusted differently because of the DNA findings? What was the target INR level? Did any of the complications occur in patients who were in the target range? Was compliance assessed? Could alcohol and drug use have affected the INR? The reported 29% reduction of re-hospitalization for bleeding or clotting complications is a relative risk. What was the absolute risk? According to a review article in American Family Physician, the median annual rate of major bleeding in patients on Coumadin ranges from 0.9 to 2.7 percent, and in this study the rate of complications in the highest risk group was only 6.3%. Complications were more likely in elderly patients, patients with co-existing illnesses, and patients with INRs outside the target range. How many of these complications could have been avoided by optimal management?
My common sense tells me patients on Coumadin can be managed just as well without knowing genetic test results. Genetic testing and pharmacogenetics hold great promise for improving individualized patient care decisions, but I don’t think Coumadin is a good example of such benefits. The DNA only confirms what our patient’s response to therapy has already told us.
![]()
“Vaccines didn’t save us” (a.k.a. “vaccines don’t work”): Intellectual dishonesty at its most naked
If there’s one thing about the anti-vaccine movement I’ve learned over the last several years, it’s that it’s almost completely immune to evidence, science, and reason. No matter how much evidence is arrayed against it, its spokespeople always finds a way to spin, distort, or misrepresent the evidence to combat it and not have to give up the concept that vaccines cause autism. Not that this is any news to readers of this blog, but it bears repeating often. It also bears repeating and emphasizing examples of just the sort of disingenuous and even outright deceptive techniques used by promoters of anti-vaccine pseudoscience to sow fear and doubt about vaccines among parents. These arguments may seem persuasive to those who have little knowledge about science or epidemiology. Sometimes they even seemed somewhat persuasive to me; that is, at least until I actually took the time to look into them.
One example of such a myth is the claim that “vaccines didn’t save us,” also sometimes going under the claim that “vaccines don’t work.” The anti-vaccine website Vaccine Liberation has a large set of graphs purporting to show that the death rates of several vaccine-preventable diseases, including whooping cough, diptheria, measles, and polio were falling before the vaccines for each disease were introduced. The the article quotes Andrew Weil:
Scientific medicine has taken credit it does not deserve for some advances in health. Most people believe that victory over the infectious diseases of the last century came with the invention of immunisations. In fact, cholera, typhoid, tetanus, diphtheria and whooping cough, etc, were in decline before vaccines for them became available – the result of better methods of sanitation, sewage disposal, and distribution of food and water.
Bill Maher has said similar things about vaccines, and the “vaccines didn’t save us” gambit has become a staple of anti-vaccine websites. For example, one particularly ignorant blogger wrote:
The mythology surrounding vaccines is still pervasive, the majority of the population still believes, in faith like fashion, that vaccines are the first line of defense against disease. The true story is that nutrition and psychological/emotional health are the first line of defense against disease.
Vaccines are a concoction of chemical adjuvants and preservatives coupled with virus fragments and have clearly been implicated in the astounding rise in neurological disorders around the world, yet the ‘popular’ media has embedded itself as a spokesperson for the pharmaceutical cartel and simply does not report in any responsible way the real situation.
Ah, yes, the “toxins” gambit! Of course, it is true that better sanitation is a good thing and has decreased the rate of transmission of some diseases for which sanitation can do so, many infectious diseases are transmitted person-to-person through the air from aerosolized drops of saliva from coughs and sneezes or from being deposited on objects that people touch frequently, like doorknobs and other fomites.
The “vaccines didn’t save us” strategy is a distortion, as I will show. The best way to demonstrate this is to go on to the very first website that currently shows up on a Google search for “vaccines didn’t save us.” Although the post is from November, it’s the main post that’s been spreading this lie since then. Entitled Proof That Vaccines Didn’t Save Us, it’s one of the most breathtakingly spectacularly intellectually dishonest bits of anti-vaccine propaganda that I’ve ever seen. I say that not because it uses a common anti-vaccine distortion, but rather because it ups the ante by adding a new one clearly designed to address the criticism of the old one. That new distortion hides it in plain sight, too, which is why I have to give the blogger props for sheer chutzpah. Actually, I have to give some backhanded kudos to the person who devised the graphs used in this post, Raymond Obomsawin, PhD. They represent the classic anti-vaccine lie, combined with some very clever cherry picking. I won’t take them all on in this post. Maybe I’ll take some of them on in a future post. In the meantime, what I will do is to take on the first several, because they represent a common anti-vaccine theme that is very similar to the one sounded by the this disingenuous post.
In fact, let’s look at the Vaccination Library claims first. Notice that there are six graphs, four of which are for vaccine-preventable diseases for which widespread vaccination was undertaken, two for which it was not. All of them show decreasing death rates from various diseases. Wow! It seems like slam dunk evidence, doesn’t it? Vaccines didn’t save us! After all, death rates were declining years before the vaccine, and they were declining for the diseases that didn’t even need a vaccine!
Death rates.
Here’s the problem. It’s not surprising that death rates were declining before introduction of the vaccines. Medicine was improving. More importantly, supportive care was improving. For example, take the case of polio. Before the introduction of the iron lung and its widespread use, for example, if a polio patient developed paralysis of the respiratory muscles, he would almost certainly die. The iron lung allowed such patients to live. Some even survived in an iron lung for decades. No doubt improved nutrition also played a role as well. However, if you want to get an idea of the impact of vaccines on infectious disease, take a look at this graph from the CDC of measles incidence, not death rates:

Similar results were seen most recently from several other vaccines, including the Haemophilus influenza type B vaccine, as the CDC points out:
Hib vaccine is another good example, because Hib disease was prevalent until just a few years ago, when conjugate vaccines that can be used for infants were finally developed. (The polysaccharide vaccine previously available could not be used for infants, in whom most cases of the disease were occurring.) Since sanitation is not better now than it was in 1990, it is hard to attribute the virtual disappearance of Haemophilus influenzae disease in children in recent years (from an estimated 20,000 cases a year to 1,419 cases in 1993, and dropping) to anything other than the vaccine.
In the post to which I referred, the most intellectually dishonest graph is this one:
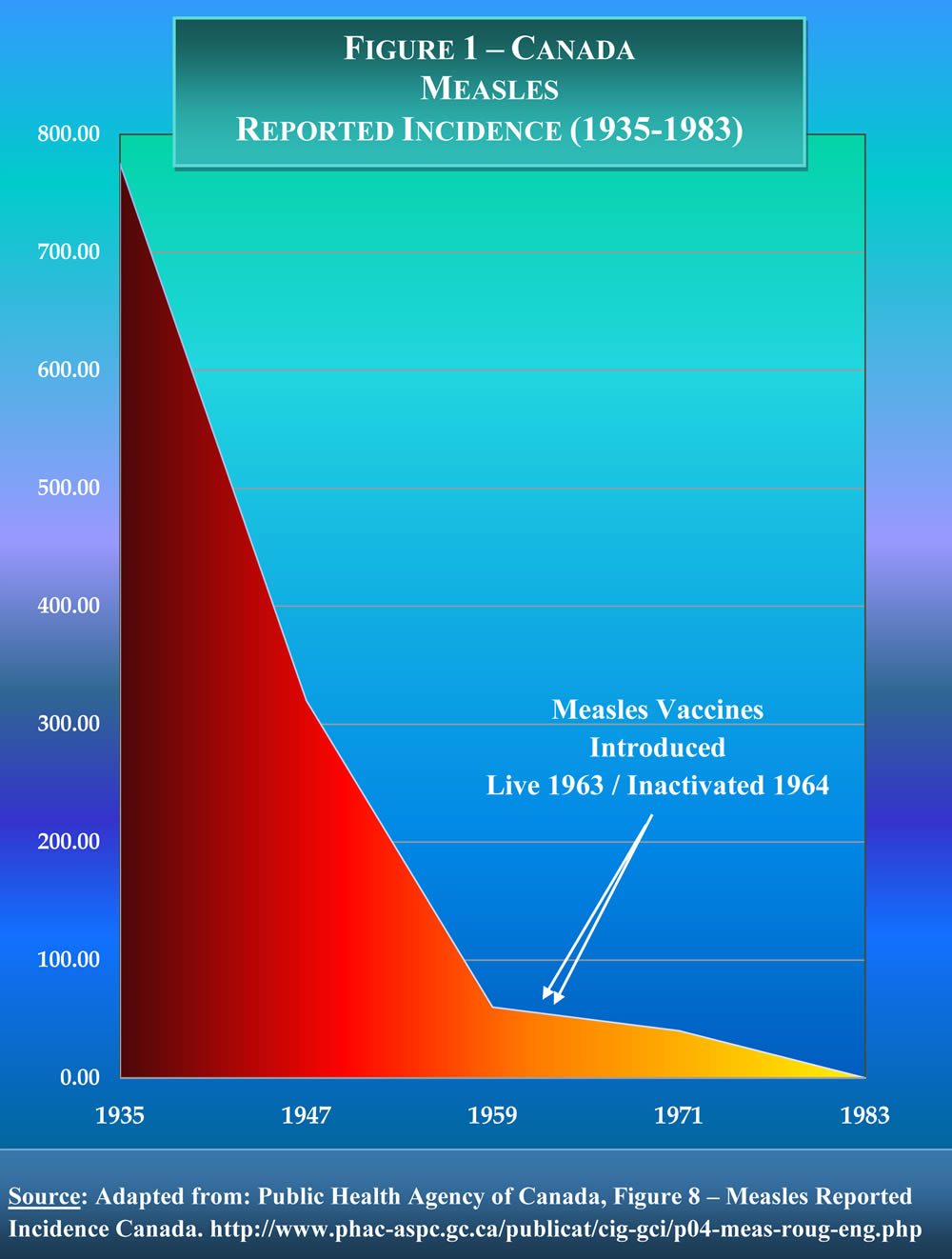
(Click to see full size figure.)
Note how this graph, unlike all the other graphs used to make the claim that “vaccines didn’t save us” actually uses incidence data, in this case from Canada from 1935 to 1983. I was immediately suspicious of this graph, though. The reason should be obvious; the decline in measles incidence is far too smooth. Measles incidence typically varies greatly from year to year. Fortunately, in his chutzpah, Obomsawin included a link to the actual source of the graph. Naturally, I couldn’t resist checking it out, and I found that the link leads to the Canadian Immunization Guide section on the measles vaccine. And this is the actual graph from which Obomsawin allegedly extracted his data:
(Click for full-sized version.)
Note how Obomsawin left out a section of ten years when measles was not nationally reportable. Also note how he has, to be charitable, cherry picked the years to produce the impression of a smoothly declining measles incidence from 1935 to 1959. As I said, it doesn’t get much more intellectually dishonest than that. But it’s even worse than that. The graph above still gives the impression that measles incidence was falling before the ten years for which there is no data. Steve Novella points out that there is a better version of the graph in this reference, and he was kind enough to send it to me, given that, for whatever reason, my university doesn’t have a subscription to the relevant journal:

(Click for full-sized version.)
Note how this graph looks at raw case numbers and shows 40,000 cases of measles in Canada the year before the ten year interruption in the data. All in all, it’s a much clearer representation of the data than the first graph, showing a clear drop that occurred during the ten year period, in the middle of which the measles vaccine was introduced. It also shows another obvious drop in measles incidence later on in the 1990s, when the two-dose measles vaccine program was started. As for why it appears that there is a steep dip in the first graph before the ten year gap, that actually appears to be an artifact. There is no data for 1959, the first year that measles was not nationally reportable in Canada, but the line appears to go to a datapoint at 1959 or 1960. My guess is that whoever made the graph decided to set the value for the beginning of the ten year gap to equal the first datapoint at the end of the ten year gap. In other words, the graph a rather poor representation of the data, and the Canadian government would do well to replace it on its website with something more like the second graph, which makes the point much more clearly.
As intellectually dishonest as Obomsawin’s graph is, this description of Obomsawin matches it:
He has produced academically and/or professionally over eighty-five (85) articles, reports, policy documents, presentations, and publications.
A search of Pubmed reveals only one peer-reviewed publication from 1978, and it’s only a commentary. In any case, apparently served as Director National Office of Health Development of the National Indian Brotherhood (AFN); Founding Chairman of NIB’s National Commission Inquiry on Indian Health; Executive Director in the California Rural Indian Health Board; Supervisor of Native Curriculum, Government of the Yukon Territory; and Evaluation Manager – Department of Indian and Northern Affairs Canada. None of these are scientific positions. More tellingly, he is “currently engaged with government funding as Senior Researcher relative to establishing a Public Sector Policy on Traditional Medicine in Canada.” My translation? He’s somehow managed to get a government grant to try to promote “traditional medicine” in Canada. Apparently, the Canadian government has its own problems with government money going to promote unscientific and pseudoscientific nonsense of the type that NCCAM promotes. In any case, besides Obomsawin’s disingenuous and intellectually bankrupt distortions of incidence data used to serve his apparently anti-vaccine agenda, he has no qualifications to speak of with regard to science or epidemiology that I can find.
It also turns out that Dr. Obomsawin has some other–shall we say?–unconventional beliefs as well. For instance, he is approvingly featured on that aggregator of all things quackery and pseudoscience, Whale.to, where he expresses anti-vaccine views, HIV/AIDS denialism, and admiration for Royal Rife. So what we have here is a woo-meister using cherry picked points on a graph to give a false impression that the measles vaccine was not responsible for the dramatic decline in measles incidence in Canada in the 1960s. Shocking, I know.
Another rebuttal to the idea that vaccines didn’t reduce the incidence of the diseases against which they were designed comes from the simple observation that, as vaccine uptake falls, the disease vaccinated against returns. Always. This is described by the CDC quite well:
Finally, we can look at the experiences of several developed countries after they let their immunization levels drop. Three countries – Great Britain, Sweden, and Japan – cut back the use of pertussis vaccine because of fear about the vaccine. The effect was dramatic and immediate. In Great Britain, a drop in pertussis vaccination in 1974 was followed by an epidemic of more than 100,000 cases of pertussis and 36 deaths by 1978. In Japan, around the same time, a drop in vaccination rates from 70% to 20%-40% led to a jump in pertussis from 393 cases and no deaths in 1974 to 13,000 cases and 41 deaths in 1979. In Sweden, the annual incidence rate of pertussis per 100,000 children 0-6 years of age increased from 700 cases in 1981 to 3,200 in 1985. It seems clear from these experiences that not only would diseases not be disappearing without vaccines, but if we were to stop vaccinating, they would come back.
The United Kingdom is an excellent illustration of this trend. Back in the mid-1990s, it declared measles as under control, thanks to the MMR vaccine. Then came Andrew Wakefield in 1998 with his trial lawyer-funded, incompetent, and possibly even fraudulent study claiming to link the MMR vaccine to “autistic enterocolitis,’ and a credulous, sensationalistic British press to spread his message that the MMR vaccine causes autism. The result was that measles came roaring back in the U.K. to the point that two years ago measles was declared endemic again there.
The Vaccine Liberation graphs and the even more deceptive graphs produced by “Dr.” Obomsawin to claim that vaccine-preventable diseases were already plummeting before the introduction of the relevant vaccines are typical of anti-vaccine arguments. First, they contain enough of a grain of truth to them to sound plausible. After all, better nutrition and better sanitation have in general contributed to better health and contributed to a decreasing toll from various infectious diseases. But they were not enough. Indeed, part of the reason we vaccinated against some diseases is because sanitation wasn’t enough. Was sanitation so much worse in the late 1980s before the Hib vaccine was introduced than it is now? No. Was it probably even that much worse in the 1960s, when the measles vaccine was introduced? Probably not. Yet, such is the myth that the anti-vaccine movement would have parents believe. Such is the intellectually dishonest nonsense they promote.
Why do they do this? J.B. Handley himself has told us why: To bring the U.S. vaccine program to its knees. Or the U.K. program. Or whatever program where the anti-vaccine program has taken hold. The reason is that, no matter how much science says it isn’t, to the anti-vaccine activist, it’s first and foremost always all about the vaccines.
![]()
The case of John Lykoudis and peptic ulcer disease revisited: Crank or visionary?
One of the themes of SBM has been, since the very beginning, how the paradigm of evidence-based medicine discounts plausibility (or, perhaps more appropriately, implausibility) when evaluating whether or not a given therapy works. One of our favorite examples is homeopathy, a therapy that is so implausible on a strictly scientific basis that, for it to work, huge swaths of well-established science supported by equally huge amounts of experimental and observational evidence would have to be found to be all in serious error. While such an occurrence is not per se impossible, it is incredibly unlikely. Moreover, for scientists actually to start to doubt our understanding of chemistry, biochemistry, pharmacology, and physics to the point of thinking that our understanding of them is in such serious error that homeopathy is a valid description of reality, it would take a lot more than a bunch of low-quality or equivocal studies that show no effect due to homeopathy detectably greater than placebo.
On Friday, Kim Atwood undertook an excellent discussion of this very issue. What really caught my attention, though, was how he educated me about a bit of medical history of which I had been completely unaware. Specifically, Kim discussed the strange case of John Lykoudis, a physician in Greece who may have discovered the etiology of peptic ulcer disease (PUD) due to H. pylori more than a quarter century before Barry Marshall and Robin Warren discovered the bacterial etiology of PUD in 1984. One reason that this story intrigued me is the same reason that it intrigued Kimball. Lykoudis’ story very much resembles that of many quacks, in particular Nicholas Gonzalez, in that he claimed results far better than what medicine could produce at the time, fought relentlessly to try to prove his ideas to the medical authorities in Greece at the time, and ultimately failed to do so. Despite his failure, however, he had a very large and loyal following of patients who fervently believed in his methods. The twist on a familiar story, however, is that Lykoudis may very well have been right and have discovered a real, effective treatment long before his time.
Kimball is right to point out that discoveries require context. Medicine can be prone to dogma. Of that, there is no doubt. Sometimes, physicians resist challenges to prevailing medical dogma. Of that, too, there is no doubt. However, reading the story of John Lykoudis, I couldn’t help but wonder the full context of his activities and efforts to convince the Greek medical authorities of the 1950s and 1960s that he was on to something. It also allows me to indulge myself in a bit of my surgical training, the bulk of which, ironically enough, occurred during the time period when the discoveries of Warren and Marshall were first revolutionizing the treatment of PUD and becoming increasingly accepted in the 1990s. When evaluating a story like that of Dr. Lykoudis and why he was unable to convince the medical profession of 50 years ago that his findings had merit, it’s very important to understand (1) the prevailing notion at the time of PUD etiology and, even more importantly, (2) how PUD was diagnosed and treated in the 1950s and 1960s.
Throughout most of the 20th century, PUD was thought to be caused by stress and dietary factors. The primary treatment for disease that had not yet developed complications was bed rest and prescription of bland diets. Towards the mid-20th century it became increasingly appreciated that gastric acid is a major factor in the etiology of PUD, and increasingly antacids, then later H2 receptor antagonists like cimetidine and ranitidine, and then still later proton pump inhibitors like omeprazole. Cimetidine and ranitidine were the mainstays of PUD treatment when I was a medical student and a resident. For complicated PUD that either was not adequately managed by drugs, sometimes surgery would be necessary. Endless were the discussions and arguments among surgeons fo the time what operation was best for PUD management, a Bilroth I or Bilroth II, vagotomy and pyloroplasty, and, at the time I was finishing my residency, the highly selective vagotomy. Then, of course, there were the discussions of what to do in the case of a bleeding ulcer that couldn’t be stopped using endoscopy or what operation to perform in the case of a perforated ulcer.
One must also remember that in the 1950s and 1960s, the diagnosis of PUD was much different than it was even in Marshall and Warren’t time in the 1980s. That’s because in the 1970s and 1980s fiberoptic endoscopy became the dominant method of diagnosing PUD. Not only did it allow for direct visualization of the ulcer, but it also allowed for potential therapy without laparotomy. More relevant for purposes of this discussion, endoscopy allows isolation of the H. pylori that causes PUD. Prior to that, the methods of diagnosis were not as accurate. In general, PUD would be diagnosed by history, physical, and then an upper GI X-ray series, in which the patient would swallow barium-containing slurries, after which fluoroscopy would visualize the stomach and duodenum.
Consequently, if you imagine yourself back in the 1950s and 1960s, the time when Dr. Lykoudis practiced, the diagnosis of PUD was less certain than it was in the 1980s. Unless it was severe, it might not even show up on upper GI series, given the limitations of the imaging technology of the time. It wasn’t always possible to distinguish between gastritis and true PUD. Consequently, a lot of diagnosis and treatment of PUD in pre-endoscopy times ended up being a lot more empiric than it is now. The diagnosis was arrived at clinically, and it was symptomatic relief that was used as the main measure of treatment success.
So what would it have taken to demonstrate, given the technology of the time, that Dr. Lykoudis’ treatment was effective? It would have taken pretty much what it would take today, minus the use of endoscopy. Consequently, we could envision a clinical trial in which standard of care at the time (bland diet, antacids, etc.) was tested against the standard of care plus Dr. Lykoudis’ antibiotic regimen. The design would be simple: Two groups, one receiving standard of care plus placebo, one receiving standard of care plus antibiotics. Alternatively, although it probably wouldn’t be considered ethically acceptable now, back in the 1960s, it probably would have been considered ethical to do an alternative study, directly comparing the then standard of care to Dr. Lykoudis’ antibiotic regimen. Whichever design were chosen, before entry in the study, each patient would have to undergo upper GI to document the presence of PUD and measure its severity. They would also have to undergo upper GI at the end of the study to document healing. Throughout the study, pain scores would be measured, and patient outcomes tracked to see what proportion of patients end up requiring surgery for their PUD and which proportion can go back to eating a regular diet. Unfortunately, Dr. Lykoudis didn’t have data anywhere near that level of rigor.
On the other hand, what I’m describing above is the equivalent of what we would call today a phase III clinical trial. In general, phase III trials aren’t started without preliminary data. But what sort of preliminary data are usually needed to provide adequate scientific justification for a phase III trial? Today, we require preclinical evidence in the form of cell culture and animal studies, as well as lesser levels of clinical evidence, such as smaller trials like phase I or phase II trials. The preclinical data provide scientific justification and plausibility, and the human data bolster that. Of course, we can’t apply today’s standards to the science of 50 years ago. Back then, the methodology and ethics of randomized clinical trials were not as advanced and well-worked out as they are today.
So what happens if we look at Dr. Lykoudis’s story and whether he might have had enough data to justify a large phase III-like clinical trial in the time in which he was practicing? By today’s standards, he probably did not. As Kimball pointed out, although plausibility does not mean understanding the mechanism, it does mean that there should be a potentially plausible mechanism, as there does not exist, for example, for homeopathy. The concept that there might be a bacterial cause of PUD is not, on the surface, incredibly implausible. But was it plausible enough to justify a clinical trial of the sort that Dr. Lykoudis proposed? What would it take? This is what Dr. Lykoudis proposed:
In 1967, Lykoudis succeeded in getting the attention of the Prime Minister’s office. His correspondence with the Minister of Health on 21 August, 1967, a sad document indeed, is revealing. He registers his frustration that medications with apparently no effect on PUD were approved, whereas Elgaco was repeatedly rejected. He proposes, in essence, a phase III trial: 100 PUD patients to be treated at a State hospital by the eminent professors, 50 with conventional treatment and 50 with Elgaco. ‘Their refusal to approve it is understandable, but their refusal to test it is not!’ he writes.
A not unreasonable assertion. Unfortunately, as Kimball pointed out, the technology to isolate and culture H. pylori didn’t exist at the time. Absent that, providing strong evidence for a bacterial etiology for PUD would require an obvious and strong response to antibiotics in the form of unambiguous symptom relief and healing documented on followup upper GI imaging studies. Even if Lykoudis had had that, he would have been unable to culture the organism responsible for PUD, which would have left scientists in a quandary. Response to antibiotics is storngly suggestive of an infectious etiology, but, absent an organism, one can never determine for sure whether it is in fact a bacteria causing a disease or the antibiotic has an activity other than its ability to kill bugs, an additional activity. For example, erythromycin increases GI motility. Thus, in the context of the time, it’s not surprising that Lykoudis’ ideas were considered highly implausible, and it would have required very strong evidence to make the idea seem plausible.
Steve Novella made a cogent observation:
But taken at face value, I think the real lesson is that process is more important than whether or not one turn’s out to be correct. Science is about process.
The problem with Lykoudis is that his behavior was indistinguishable from the myriad quacks and charlatans that existed then and exist today. That in hind sight one turned out to be on the right track is not all that surprising, and their contemporaries should not be faulted for their inability to predict the future.
The question is – what did Lykoudis do to convince the scientific community of his claims. Did he perform carefully controlled double-blind placebo-controlled trials? Did he attempt to enlist the help of a microbiologist to try to isolate the organism? Or did he just expect people to take his word for it?
What did he do to deserve being taken seriously? Being right in the hindsight of history is not enough.
And I think that this is the key point. Science is a process. It is by its very nature constrained by what is known at any given time in history. In the context of Dr. Lykoudis’s time and given what was known then, it is not surprising that his idea would have encountered heavy resistance from the scientific orthodoxy of the time. Another issue to consider is regional variation in physicians’ attitudes. One example I like to use to illustrate this is the reaction of European physicians to the ideas of Ignaz Semmelweis. Semmelweis, as most readers will recall, first demonstrated that the high rate of puerperal fever in the obstetrics ward run by physicians was due to physicians not washing their hands after doing autopsies, going straight from the morgue to the delivery room. Semmelweis’ findings were far more favorably received in England, for example, than they were on the continent. It is possible, although by no means assured, that Lykoudis’ ideas might have been better received if he had lived in a different part of the world.
Here’s one final consideration. Science is performed by human beings. Although it is a process designed to overcome human biases, communicating the results of scientific research is subject to the same idiosyncracies to which any human communication is subject. Anyone who’s ever been to a scientific conference knows that. It is quite possible to be right and, to put it bluntly, to piss off the very scientists that need to be convinced so much that they harden their positions protecting the scientific consensus. One example is Semmelweis himself. Sherwin Nuland, in his book The Doctors’ Plague: Germs, Childbed Fever and the Strange Story of Ignac Semmelweis, suggested that if Semmelweis had communicated his findings more effectively and managed not to antagonize the medical establishment so thoroughly he might not have been marginalized and dismissed in the manner that he was. At the very least, he may not have been met with as much hostility. Galileo, although apparently not intentionally, alienated the Pope at the time by putting his words in the mouth of a character named Simplicio defending the Aristotelian Geocentric view in Dialogue Concerning the Two Chief World Systems. Reading between the lines, one can see echoes of this sort of antagonism in Lykoudis’s story. Indeed, Michael Phillips of St. Vincent’s Medical Center wrote in an letter to The Lancet:
I propose a less dramatic metaphor: medicine is a marketplace of ideas, with sellers and buyers. Sellers (innovators with new ideas) advertise their intellectual property to potential buyers (other physicians). This buying public is highly sophisticated and sceptical. Quite correctly, physicians will only accept the highest quality new ideas because the lives of their patients are at risk. So physicians buy only when they see the hallmark of quality: publication in a respected peer-reviewed journal.
That in a nutshell explains the tragedy of John Lykoudis. He had a wonderful intellectual product: the insight that peptic ulcer disease is infectious, supported by the evidence that it can be cured with antibiotics. But he lacked the ability (or the training) to sell this insight to his colleagues. He was a retail trader who treated individual patients instead of targeting the wholesale market of other physicians.
Of course, this is the problem. Most physicians are not scientists, and many physicians are very prone to being swayed by anecdotal evidence. Without well-designed clinical trials based on the best basic and translational science available, way to validate or refute anecdotal data. I find Lykoudis’s story to be a cautionary tale. Whether he was correct and thus the true “Galileo” of H. pylori, rather than Warren and Marshall or whether he was just another crank, his story demonstrates that we scientists should be very careful to guard against excessive smugness. As has been repeated by many skeptics in many variants over the years, it is not sufficient to claim the mantle of Galileo as a persecuted martyr for science. You must also be right. Even though it is not clear whether, taken in the context of the time, Lykoudis was a crank or a misunderstood physician who was ahead of his time, Warren and Marshall’s vindication of his ideas that PUD is bacterial in etiology reminds us that not all who claim the mantle of Galileo are necessarily cranks. The vast majority usually are, but on very rare occasions we do see a real Galileo.
![]()
Brief Note: Followup on Spinal Decompression Machines
In September 2008 I wrote a post on Misleading Ads for Back Pain Treatment. with particular attention to the bogus claims for the DRX 9000.
The Canadian Broadcasting Company (CBC) show “Marketplace” has just done a scathing exposé of so-called nonsurgical spinal decompression treatment with machines like the DRX 9000 and of some of the unscrupulous practitioners who offer it. Between the hidden camera footage and the weasel words of the chiropractor they interview, it’s quite entertaining.
![]()
What does the Health Care Freedom of Choice Act actually do?
 The Act is sponsored by the American Legislative Exchange Council,(ALEC) a coalition of conservative, moderate and libertarian state legislators who support "Limited Government, Free Markets and Federalism."
The Act is sponsored by the American Legislative Exchange Council,(ALEC) a coalition of conservative, moderate and libertarian state legislators who support "Limited Government, Free Markets and Federalism."
The main objectives of the legislation:
• Ensuring Access to Health Services—Without Waiting Lists. When consumers control the dollars, they make the decisions. On the other hand, a single-payer health care —which forces patients to enroll in a one-size-fits-all plan with rich benefits and weak cost-sharing—will cause spending to skyrocket and policymakers to ration care as a cost-containment measure.
• ALEC's Freedom of Choice in Health Care Act ensures a person's right to pay directly for medical care. Single-payer systems, like in Canada, make it illegal for citizens to go outside the government's health care plan and contract for their own medical services. Cost overruns require most single-payer plans to restrict patient choices, and instead mandate an "evidence-based" treatment schedule that standardizes care.
• ALEC's Freedom of Choice in Health Care Act would block legislation that imposes costly, bureaucratic penalties for choosing to obtain or decline health coverage. This provision strikes at the heart of an individual mandate—implemented in Massachusetts and elsewhere—that penalize individuals and businesses for failing to purchase health insurance.
Where does it stand?
According to ALEC, legislation has been filed in 35 states:
Alabama, Alaska, Arizona, Arkansas, Delaware, Florida, Georgia, Idaho, Illinois, Indiana, Iowa, Kansas, Kentucky, Louisiana, Maryland, Michigan, Minnesota, Mississippi, Missouri, Nebraska, New Hampshire, New Jersey, New Mexico, North Dakota, Ohio, Oklahoma, Pennsylvania, South Carolina, South Dakota, Tennessee, Virginia, Washington, West Virginia, Wisconsin, and Wyoming. (Arizona's HCR 2014, a revised version of the ALEC model, will be put on the ballot in 2010.)
The legislation has since passed and been signed into law in Idaho, and is on the verge of becomming the law of the land in Virginia and Oklahoma.
In Texas there are calls for Gov. Rick Perry to call a special session of the legislature for HCFCA.
Blue Collar Republican files for MO State Rep. against his own Wife
 Livin' Lovin'... Heartbreaker??
Livin' Lovin'... Heartbreaker??
From Cliff Thies:
Missouri state Representative Linda Fischer, a Democrat, is running for re-election this November. She is being challenged by her husband, John Fischer, who has re-registered as a Republican.
This might be funny if it weren’t so sad. The two are involved in a messy court proceeding. Their marriage was probably already over. Also, Mr. Fischer had been formerly employed for almost thirty years in Chrysler Corporation automobile assembly plants, before he took early retirement.
 He was just a Regular Joe forklift drive; she a powerful state legislator
He was just a Regular Joe forklift drive; she a powerful state legislator
He says he is running for the workers of Missouri and, actually, this could be true. Our economy is in a shambles. A lot of people are hurting. Workers, small business, investors, people in our cities and our rural places, people reflecting the great diversity of our country.
From KMOV.com:
"I figured if I'm going to be on my own, then I'm going to have to do what suits me," he said. "I'm standing up for people who lost their job. I don't think they're being represented fairly in this state because they do not take care of the working man."
We need leaders who speak to our shared interest in reviving our economy, not people who speak about redistributing of what remains of our wealth.
In Missouri District 107 (east central MO - Bonne Terre) Vote Republican!
Does Libertarian for NY Gov. Kristin Davis, have a bit of a "conservative" streak?
 From Eric Dondero:
From Eric Dondero:
Former Manhattan Madame, and media celebrity Kristin Davis, currently seeking the Libertarian nomination for New York Governor, issued a press release Wednesday, praising California's initiative to legalize marijuana.
Said Davis:
"Californian's have figured out what New Yorker's need to figure out. Marijuana is a $10 billion a year industry in New York State. Its legalization and taxation will help New York's current financial crises."
But in an interview with NY NewsBlaze, Davis took a very unique approach to legalization, giving it a bit of a conservative twist.
From NewsBlaze:
Davis said she would strongly support an Opt-Out clause where localities could opt by local vote not to sell marijuana in that locality. "I believe in home rule and local option. Some counties may choose to allow legal pot sales, others may not."
Such a view could come as a relief to more socially conservative Upstate towns and localities. And could win her some critical Upstate voting support.
POLL SHOCKER FROM ZOGBY!! Democrats now backing away from Israel; Republicans overwhelmingly support Jewish State
 92% of Republicans on Israel's side; only 42% of Democrats
92% of Republicans on Israel's side; only 42% of Democrats
From Eric Dondero:
In 2008, 78% of all American Jews voted for Barack Hussein Obama for President. Many of the 22% of Jews who voted against him, warned of a coming catastrophe in American foreign policy against Israel, if he were to be elected. The 22% have proven to be correct:
• Obama administration pushback against Israeli warnings over the threat of an Iranian nuclear arsenal.
• Benjamin Netanyahu insulted by Obama at a recent White House visit. Obama walked out of the room in the middle of their meeting, with the excuse, I'm going to have dinner "with Michele and the kids."
• The very latest; threats by the US to vote "present" for the very first time, in the UN Security Council against Israel, in regards to calls to halt further Israeli housing in East Jerusalem.
And now this breaking news from Zogby:
The poll’s findings also highlight the deep partisan gap that continues to grow between Republicans and Democrats, with Democrats having an unfavorable rating of Israel for the first time.
•42% of Democrats had a favorable rating of Israel compared to 92% of Republicans resulting in a 50% gap between the parties.
•While the gap is higher in this poll, the finding is consistent with a recent Gallup poll that had 53% of Democrats with a favorable view compared to 80% of Republicans.
Will this help Republican candidates with the Jewish community heading into the November elections?
Despite repeated attempts, pollster John Zogby was unavailable to provide Libertarian Republican with a comment on this question.
However, Joe Sciarrino, Spokesman for the National Republican Congressional Comm. commented to LR:
"The United States has had a long-standing and strategic partnership with Israel, and over the past year we’ve seen this Administration neglect that relationship. Democrats in Congress who agree with this decision to alienate such a key ally may risk alienating voters come November.”
Photo Minn. Cong. Michele Bachmann addressing the Republican Jewish Coaltion.
Public Sector employees causing Higher Private Sector Unemployment
NEW FROM REASON TV!
Nick Gillespie, Reason Editor, looks at the economic pie, and how the increasing size of public sector employment is causing private sector employees to lose jobs.
Noted: Public sector employees now make about $8,000 more than their private counterparts.
More than 8 million private sector jobs have been lost in the Obama recession, while the public sector saw a net gain of at least 100,000 jobs.
Georgia Senate overwhelmingly passes Health Care Freedom of Choice Act
 All Republicans vote in favor
All Republicans vote in favor
If this is not repealed "there will be virtually no activity by a state, a citizen, or a business that the feds would not someday be able to regulate." -- Bob Barr, 2008 Libertarian Presidential candidate
From Eric Dondero:
Encouraging news out of Georgia. The State Senate has just passed the Health Care Freedom of Choice Act by an overwhelming margin of 31 to 17. All Republicans voted for the measure. They were joined by only one single Democrat.
The bill was sponsored by members of the Georgia Senate Liberty Caucus, including Sen. Judson Hill of Marietta who called it the "best way to protect Georgians from the Democrat-led Congress' attempt to socialize health care through their public option health care mandate."
From Quarterdeck blog:
Georgia Senator Judson Hill (photo) was joined by 29 other Senate Republicans last Thursday passing legislation protecting Georgians’ rights to choose their own health care. Senator Hill authored Senate Bill 317 and has been working the past year to prohibit any government, state or federal, from forcing its citizens to participate in any health care system.
Under Senate Bill 317 Georgia’s citizens would be protected from being forced by the government to purchase health care.

The Bill now goes on to the House. Republican Governor Sonny Perdue is fully expected to sign the law once it passes the House.
Fmr. Georgia Republican Congressman and 2008 Libertarian Presidential candidate Bob Barr wrote in the Atlanta Journal-Constitution "States must challenge Health Care law":
Governor Sonny Perdue, for example, worries how the Peach State will fund what he estimates will be an additional billion dollars of Medicaid spending each year. Private companies, which will be subject to numerous mandates by virtue of the law, face daunting fiscal challenges as well.
Governor Perdue has indicated he will pursue a challenge using lawyers other than the state attorney general, [Democrat] Thurbert Baker, who has refused to lend his office and his name to the project. Perdue, unlike Baker, correctly understands the importance of such a lawsuit; for if the federal government is permitted to enforce mandates such as those in this new law, then there will be virtually no activity by a state, a citizen, or a business that the feds would not someday be able to regulate.
For a full list of GA Senate Liberty Caucus members visit GARLC.org
The Thomas Jefferson Question: Interview with Texas Freedom Network’s Dan Quinn over Textbook controversy
 FROM THE EDITOR: Libertarian Republican was fortunate to have the opportunity to interview Dan Quinn, Communications Director, Texas Freedom Network on the recent Textbook controversy concerning the Texas Board of Education. We appreciate Mr. Quinn taking the time to answer these important questions that greatly affect liberals, conservatives and libertarians.
FROM THE EDITOR: Libertarian Republican was fortunate to have the opportunity to interview Dan Quinn, Communications Director, Texas Freedom Network on the recent Textbook controversy concerning the Texas Board of Education. We appreciate Mr. Quinn taking the time to answer these important questions that greatly affect liberals, conservatives and libertarians.
LIBERTARIAN REPUBLICAN: Mr. Quinn, Texas Board of Education members are disputing your assertion that Jefferson was removed from history textbooks. Gail Lowe and Cynthia Duncan have said in national interveiws that what actually happened is that discussion of TJ was moved from the Enlightenment period to the American Revolution. Do you care to dispute that fact?
DAN QUINN: We haven't asserted that the board removed Jefferson from history books. From our live-blogging of the meeting on March 11:
9:27 – The board is taking up remaining amendments on the high school world history course
9:30 – Board member Cynthia Dunbar wants to change a standard having students study the impact of Enlightenment ideas on political revolutions from 1750 to the present. She wants to drop the reference to Enlightenment ideas (replacing with “the writings of”) and to Thomas Jefferson. She adds Thomas Aquinas and others. Jefferson ’s ideas, she argues, were based on other political philosophers listed in the standards. We don’t buy her argument at all. Board member Bob Craig of Lubbock points out that the curriculum writers clearly wanted to students to study Enlightenment ideas and Jefferson . Could Dunbar’s problem be that Jefferson was a Deist? The board approves the amendment, taking Thomas Jefferson OUT of the world history standards
9:40 – We’re just picking ourselves up off the floor. The board’s far-right faction has spent months now proclaiming the importance of emphasizing America ’s exceptionalism in social studies classrooms. But today they voted to remove one of the greatest of America ’s Founders, Thomas Jefferson, from a standard about the influence of great political philosophers on political revolutions from 1750 to today
9:45 – Here’s the amendment Dunbar changed: “explain the impact of Enlightenment ideas from John Locke, Thomas Hobbes, Voltaire, Charles de Montesquieu, Jean Jacques Rousseau, and Thomas Jefferson on political revolutions from 1750 to the present.” Here’s Dunbar ’s replacement standard, which passed: “explain the impact of the writings of John Locke, Thomas Hobbes, Voltaire, Charles de Montesquieu, Jean Jacques Rousseau, Thomas Aquinas, John Calvin and Sir William Blackstone.” Not only does Dunbar ’s amendment completely change the thrust of the standard. It also appalling drops one of the most influential political philosophers in American history — Thomas Jefferson.
From our March 12 press release:
"Even as board members continued to demand that students learn about "American exceptionalism," the board stripped Thomas Jefferson from a world history standard about the influence of Enlightenment thinkers on political revolutions from the 1700s to today. In Jefferson 's place, the board's religious conservatives succeeded in inserting Thomas Aquinas and John Calvin. They also removed the reference to "Enlightenment ideas" in the standard, requiring that students should simply learn about the influence of the "writings" of various thinkers (including Calvin and Aquinas)."
We repeated that paragraph in a March 13 blog post summarizing the worst changes the board made:
And if you check our other blog entries, you will note that we have been careful to explain that Jefferson was deleted from that world history standard, not from the "history books."
LIBERTARIAN REPUBLICAN: Mr. Quinn, as you probably know, Thomas Jefferson is a great hero to libertarians. Initially, we libertarians were quite concerned that conservatives were reported to have removed him from history textbooks. In fact, many of us were outraged. But after learning the truth of the matter, our outrage turned to liberal bloggers who initially mis-reported the story. Could you clarify for us the origination of reports that Jefferson had been removed from history textbooks? Did TPM and other liberal bloggers just miscontrue the facts, or were they purposely trying to split libertarians from conservatives by spinning the news?
DAN QUINN: If others have misreported what happened, you'll have to talk with them. But keep in mind that other bloggers were not at the meeting and in many cases were relying on possibly imprecise reports from elsewhere -- much as conservative bloggers were reacting to false reports last year that Christmas had been taken out of social studies textbooks in Texas . Sadly, some people are permitting Lowe and Dunbar to distract them with a red herring. This isn't a contest about how many times Jefferson is listed in the standards, whether those references are in American history or elsewhere. The question is why board members don’t want students to learn that Jefferson, who argued (among other things) that a "wall of separation between church and state" as essential to freedom, was an influential Enlightenment thinker who inspired people around the world struggling for freedom. Moreover, why did the board change the thrust of the standard altogether by removing even the reference to the Enlightenment and replacing Jefferson with Thomas Aquinas, John Calvin and William Blackstone? We have been monitoring this board for 15 years, and the answers to those questions are certainly no mystery to us. This board is controlled by a faction that is hostile to the separation of church and state. In fact, during the same meeting they rejected a proposed standard that would have required students to “examine the reasons the Founding Fathers protected religious freedom in America by barring government from promoting or disfavoring any particular religion over all others.” The board knew that removing other references to Jefferson would be politically impossible. But removing him from a standard about the influence of his ideas on people struggling for freedom around the world, they thought, would be easier. Moreover, it doesn't surprise us in the least that this board would want to water down the influence of Enlightenment thinking on political revolutions from the 1700s to the present. Enlightenment philosophies run counter to their own worldview.
LIBERTARIAN REPUBLICAN: As you're probably aware, a great many libertarians are Darwinists, even Social Darwinists, and are not comfortable with some of the more extreme elements of the Religious Right. We are concerned that some religious conservatives might seek to give parity to Darwinism with theories based on a Creationist view. However, given the misreporting of the Jefferson story, and the misinformation put out by liberal groups based mainly in Austin , how should libertarians trust such reports in the future?
DAN QUINN: As in all things in life, choose your sources carefully, and be particularly wary of politicians spinning wildly in an attempt to justify the indefensible. I note that you mention Talking Points Memo specifically. This is what TPM reported:
TPMMuckracker.talkingpointsmemo.com
“According to TFN: ‘the board stripped Thomas Jefferson from a world history standard about the influence of Enlightenment thinkers on political revolutions from the 1700s to today. In Jefferson 's place, the board's religious conservatives succeeded in inserting Thomas Aquinas and John Calvin. They also removed the reference to 'Enlightenment ideas' in the standard, requiring that students should simply learn about the influence of the 'writings' of various thinkers (including Calvin and Aquinas).”
You didn’t mention Huffington Post, but they reported essentially the same thing, linking back to our blog:
Part of the problem here is that Lowe, Dunbar and their supporters want everyone to believe that the bulk of the reporting on what they did has been inaccurate. In fact, much of it hasn’t been. But it serves them to suggest that the reporting has been inaccurate because then bloggers will challenge their critics for supposedly being untruthful. On this point, I highly recommend the following piece:
In short, trusting what you hear from these state board members is perilous.
Regarding science, this board did, in fact, insert creationist/"intelligent design" arguments into our science standards last year in an attempt to challenge the validity of evolutionary theory. One such argument has students study whether the fossil record supports evolutionary theory. The other has students study the complexity of the cell to decide whether natural selection could account for changes in the development and diversity of life. Both are textbook creationist/"intelligent design" arguments ("gaps in the fossil record," "irreducible complexity").
LIBERTARIAN REPUBLICAN: Thank you very much for your time Mr. Quinn.
Liberal Columnist Howard Fineman warns Democrats in for "Colossal losses"
Howard Fineman of NewsWeek offers a stunning assessment of Democrats chances for Congress: After surveying the latest polls on Health Care, Fineman finds that the Dems may be in for spectacular losses in November.
From NewsWeek "The numbers don't lie":
On the day the president signed into law the "fix-it" addendum to the massive health-care measure, two new polls show just how fearful and skeptical Americans are about the entire enterprise. If the numbers stay where they are—and it's not clear why they will change much between now and November—then the Democrats really are in danger of colossal losses at the polls.
The first week of salesmanship by the Democrats and the president hasn't done any good. According to the new Rasmussen poll, only 41 percent of Americans think the law is "good for the country," compared with 50 percent who see it as "bad for the country." Last week the ratio was 41–49 percent. Sixty percent think the measure is "likely to increase the deficit"—also a figure unchanged from last week.
In Gallup's new poll... Americans think the law will harm the U.S. economy (44–34 percent), the overall quality of health care in the U.S. (55–29 percent), and the federal balance sheet (61–23 percent).
Fineman also quotes an un-named Democratic Senator who called the bill "political folly."
(H/t Memeo)
Libertarian Wayne Root to Larry King: Yes, Abolish Social Security

 Republicans who defend SS risk losing votes to Libertarian, Tea Party
Republicans who defend SS risk losing votes to Libertarian, Tea Party
From Eric Dondero:
While mainline Republicans are defending Medicare and Social Security, a growing number of disaffected Tea Party Patriots and Libertarians are saying "hold on a minute!" We actually do want to abolish the program, or at the very least privatize it through a gradualist approach.
The Libertarian Party, which originated the Tea Party protests in 2008, has long advocated abolishment of Social Security.
From the LP Platform:
Retirement planning is the responsibility of the individual, not the government. We favor replacing the current government-sponsored Social Security system with a private voluntary system. The proper source of help for the poor is the voluntary efforts of private groups and individuals.
On Monday night, 2008 Libertarian Vice-Presidential candidate, and potential 2012 LP Presidential standardbearer Wayne Root appeared on Larry King. He was joined by local St. Louis Tea Party leader Dana Loesch, who has increasingly become a media spokesman for the nationwide Tea Party movement.
Partial transcript from YouTube video:
KING: We had to pay Social Security. That was a socialist concept. Republicans voted against it at the time.
LOESCH: Oh, I agree. Yeah.
KING: Would anyone turn away Social Security now? Would you do away with it?
LOESCH: I would, yeah.
KING: Would you do away with it?
LOESCH: Yes.
KING: Would you do away with it Wayne?
ROOT: Well, I'd certainly like to. At best I'd do away with it, cause I could find better ways to save and invest my own $15,000 a year... If you put it up for a vote today a majority would want to keep it, but they'd certainly want to privatize a small portion of it... I think I can do better with my $15,000 a year, and I'd like it to be mine. It's mine.
Mainline Republicans who continue to defend failed government entitlement programs risk losing votes to Libertarian Party candidates in 2010. A loss of 3 to 4% in a close Congressional race for instance, to a Libertarian candidate who is advocating privatization, could prove disastrous to many GOP campaigns.
Don’t Just Say “No”
Voters!
You must step back and look at the big picture.
You must look at the actions and not the words of our current one party political system.
The big picture is that both the Republicans and Democrats mean to grow government and control your lives in ways that were unimaginable even 20 years ago. They are now [...]
Jason Kilar Leads Hulu To Profitability, But Will He Stay On At Hulu? – TVbytheNumbers
 TVbytheNumbers | Jason Kilar Leads Hulu To Profitability, But Will He Stay On At Hulu? TVbytheNumbers If Hulu can extract more ad revenue for an hour of viewing, the FX's of the world may upload more shows onto the Web site. Already some of Hulu's commercial ... |