
If there’s one thing that’s true of the human race, it’s that when it comes to persuasion language is has power. Words have power. Just ask the advertising industry or politicians, who rely on their skills manipulating language to persuade for their very livelihood and authority. In the specific bailiwick of this blog, Science-Based Medicine, many of us have spent considerable verbiage describing how advocates of unscientific modalities rebranded as “complementary and alternative medicine” (CAM) and/or “integrative medicine” (IM) are incredibly skilled at the manipulation of language and renaming of terms in order to make them sound more persuasive, particularly to make it sound as though their modalities are scientifically supported or that it’s just another “alternative” to SBM. In fact, Kimball Atwood has made a special study of the language of CAM, even going so far to do an amusing feature that he used to call the Weekly Waluation of the Weasel Words of Woo. Indeed, the very name “integrative medicine” is a masterful term that makes it sound as though they’re just “integrating” the best of scientific medicine and “traditional” or “alternative” medicine when in fact what is happening all too often is the “integration” of quackery with medicine or, as I sometimes like to call it, “integrating” fake medicine with real medicine. Unfortunately, my definition of “integrative medicine” doesn’t appear to be winning, although I was gratified that I got several Tweets during our panel at TAM9 quoting my line about integrating quackery with medicine.
The anti-vaccine movement has been pretty good, albeit not as masterful as, say, Andrew Weil, when it comes to manipulating language to its own end. Who can forget three years ago, when the meme started spreading throughout the anti-vaccine movement that it’s “not anti-vaccine but rather ‘pro-safe vaccine’” and started demanding that the government and pharmaceutical companies “green our vaccines.” The reason is obvious; even anti-vaccine activists know that it’s a public relations loser to be explicitly anti-vaccine, which is Jenny McCarthy and the anti-vaccine groups that participated in her “Green Our Vaccines” rally did their best to downplay and hide their radical anti-vaccine base. They failed. (The signs about vaccines as “weapons of mass destruction” rather undercut the “pro-safe vaccine” message. I’ve dealt with this fallacy before in depth, explaining why it is appropriate to call them “anti-vaccine,” even as they strenuously deny that they are. More recently, the preferred narrative has been “too many, too soon,” which leads me to another term coined by the group SafeMinds and promoted on—where else?—Age of Autism.
Now, the SafeMinds/AoA approach is being dubbed “SmartVax.”
The Orwellian language of the anti-vaccine movement
I have to hand it to the anti-vaccine movement in general and SafeMinds in particular. I really do. Whatever the deficiencies in their knowledge of science, anti-vaccine advocates sure can spin the Orwellian language, where up is down, left is right, and vaccines are alway, always, always the cause of autism, or at least more harmful than good. The first stroke of propaganda genius about this site is the term “SmartVax” itself. Yes, it’s painfully obvious. After all, who wants to be in favor of the implied opposite of “SmartVax,” such as “DumbVax” or “StupidVax”? Of course, I fervently hope that some day a vaccine against dumb and stupid will one day be invented, but most likely I hope in vain. If there is one thing that isn’t vaccine-preventable, it’s stupidity. Yet that’s not the propaganda genius, at least not in and of itself. What elevates the dreck on the SmartVax website into the realm of brilliant P.R. is how the anti-vaccine activists contrast “SmartVax” with what they call “MaxVax.” Let’s take a look, shall we? It begins with a bit of revisionist history in a section entitled Overview of the SmartVax Philosophy:
In the early 1900′s, scientists coined the terms “allergy” and “anaphylaxis” to describe vaccine-injuries; at present, the mechanism by which vaccines cause injury is still not scientifically understood. Historically, the vaccine-injury risk has caused vaccine manufacturers and public health officials to be conservative when recommending new vaccines or administration of vaccines at earlier ages. However, vaccines proved effective against some deadly diseases and by the 1970′s a “maximize vaccination” philosophy arose that viewed vaccines as always having more benefits than risks.
Not exactly. The assertion that scientists coined the terms “allergy” and “anaphylaxis” to describe vaccine injuries is a distortion, with one minor grain of truth. Let’s start with the term anaphylaxis, the coining of which had nothing to do with childhood vaccines. Rather, it derived from the studies of Charles Richet and Paul Portier over 100 years ago of the toxin produced by a jellyfish, the Portuguese Man of War. During an oceanographic expedition, Richet and Portier managed to isolate the toxin and thought that they might be able to use the toxin in order to obtain protection, or, as they called it, “prophylaxis” in order to protect swimmers who came into contact with the jellyfish. When they returned to France, they didn’t have access to the jellyfish anymore; so they turned their attention to the toxin produced by the sea anemone Anemona sulcata, the “sea nettle”, which could be harvested in large quantities from the Mediterranean Sea. They injected venom from the sea nettle at various doses into dogs. The dogs that survived were allowed to recover and then reinjected. To their surprise, subsequent small doses of the toxin produced a dramatic illness that resulted in difficulty in breathing followed by rapid decline and death. Richet and Portier called this reaction “anaphylaxis,” meaning “against protection.” They concluded correctly that the immune system becomes sensitized to the toxin and that re-exposure to the same substance could result in a severe reaction, a discovery for which Richet won the Nobel Prize in Physiology or Medicine in 1913. Vaccine injury is not exactly the same thing as what the SmartVax website is referring to.
SafeMinds is also distorting the history of the term “allergy,” which actually was not coined to describe vaccine “injuries.” Rather, the term “allergy” was first coined in 1906 by Clemens von Pirquet. A year earlier, von Pirquet studied the describe adverse reactions of children who were given repeated shots of horse serum to fight infection. Here’s a hint: Injecting horse serum to fight infection is not the same thing as being vaccinated. Indeed, Emil Adolf Behring won the Nobel Prize in Physiology or Medicine in 1901 for the development of the diptheria antitoxin, having observed that injecting extracts of diptheria cultures containing diptheria toxin into an experimental animal induced the animal to produce something in its serum that could protect another animal against infection with diptheria. Ultimately, this led to a treatment for humans in which horse serum antitoxin was used in order to treat and prevent the disease, but unfortunately proteins in the horse serum could at times result in allergic reactions upon repeated doses. The following year, the term allergy was proposed to explain this unexpected “changed reactivity” in response to exposure to the horse serum. Later, in 1907 Pirquet characterized the same effect due to repeated doses of the smallpox vaccine–after he had coined the term for his previous observations.
After that little paragraph of revisionist history follows more revisionist history that consists largely of confusing correlation with causation (the “autism epidemic” that isn’t), claiming that the anti-vaccine groups that arose during the 1980s advocated a “smarter” vaccine schedule, and pointing out the 1986 law that created the National Vaccine Injury Compensation Program without mentioning that anti-vaccine grande dame Barbara Loe Fisher was a driving force behind the passage of that law. Anti-vaccine groups only turned on the law when they didn’t like how the Vaccine Court had the temerity to try to use actual science to determine what does and doesn’t constitute a true vaccine injury. It didn’t matter that the Vaccine Court bent over backwards to give parents the benefit of the doubt, that it came up with a list of “table injuries” that are presumed to be due to vaccines even when the evidence is somewhat questionable, and that it paid most legal fees fo its petitioners, whether they won or lost. When the Vaccine Court didn’t accept the pseudoscientific view that vaccine injuries cause autism, the anti-vaccine movement turned on it and now generally rant that the requirement that vaccine injury claims go through this special court has allowed vaccine manufacturers to avoid any accountability. Never mind that the FDA and FTC regulate them and that the regulations covering pharmaceutical products (like vaccines) require considerably testing and oversight.
The revisionist history here didn’t exactly make me confident in anything else on this website, but let’s move on. Here is where we get to the meat of the matter; this is what SafeMinds describes as the difference between what it calls the “SmartVax” and the “MaxVax” philosophies:
SmartVax and Max-Vax are both “pro-vaccine” philosophies, in that both philosophies consider vaccines an important component in an overall children’s health program, but SmartVax differs from Max-Vax in important aspects of safety, research, and policy. The SmartVax philosophy is all about being smart with vaccinations: don’t over-use them, don’t bypass good science, understand the risks, and ensure that the risks are not hidden from the public.
Uh, no. Not even close.
Does SafeMinds really think we’re stupid enough to believe that its philosophy is in any way “pro-vaccine”? Think about it this way? Have you ever seen SafeMinds advocate the routine use of any vaccine or defend any vaccine? I certainly haven’t, and I’ve scoured its website looking for such a statement. What I see instead are unending claims that vaccines are unsafe or haven’t been adequately tested based on misinterpretation and cherry picking of studies, fear mongering, and rejection of studies failing to find a link between vaccines and autism almost before they are published. Just type the word “SafeMinds” into the search box in the upper left hand corner of this page, and you’ll see copious evidence of the anti-vaccine activism of SafeMinds, including, most recently, its purchasing public service announcement time in AMC Theaters for its anti-vaccine message, which, not surprisingly, has led to complaints of “censorship” and conspiracy theories about big pharma, pediatricians, and the government trying to shut SafeMinds down. That’s hardly about “not bypassing good science,” which is exactly what SafeMinds does every time it trashes studies that fail to find a link between vaccines and autism.
Basically, SafeMinds contrasts its “SmartVax” (i.e., its anti-vaccine policy in disguise) with “MaxVax” (what it labels the current vaccine schedule) by two “pillars”:
- Evidence-Based Scientific Research (go where the evidence leads)
- Appropriate Checks-and-Balances on Vaccine Policy
Pillar one is based on a delusion coupled with a massive straw man:
The first rule of SmartVax is the pursuit of evidence-based scientific research on vaccine-injuries to an unbiased conclusion, without being afraid of what the evidence might show, to develop the knowledge for a safer and more effective vaccine program in the long-term. This is in stark contrast with the Max-Vax tenet that such research should be avoided because the results might undermine public confidence in the current vaccine program.
The delusion is, of course, that SafeMinds or any other anti-vaccine group does or advocates anything resembling unbiased, evidence-based research. Quite the opposite, as we’ve documented time and time again over the last three years right here on this very blog, for example here. The straw man is that scientists claim that research should be avoided because the results might undermine public confidence. A more accurate and honest representation of the Orwellian-named “MaxVax” position would be that a link between vaccines and autism is highly implausible and that, although it is impossible ever to prove a negative completely (i.e., that there is absolutely no link between vaccines and autism), enough studies have been done to estimate the chances of such a link existing to be very, very, very low. After all, even Generation Rescue’s attempts at finding a link between vaccines and autism have failed utterly. In actuality, it is SafeMinds and its ilk that require more and more such research for the very purpose of undermining public confidence in the current vaccine program; that’s the raison d’être of anti-vaccine groups. And, of course, the “MaxVax” moniker itself is a not-so-subtle attempt to paint the public health establishment with the brush of unreasoning extremism and dogma.
Here’s pillar two:
The SmartVax view holds that appropriate checks-and-balances on vaccine policy will produce the most beneficial vaccine program long-term for children’s health. Government-owned research data on vaccine-injuries should be made open to the public and easily accessible to all researchers. Long-term double-blind placebo studies tracking both acute and chronic health conditions (e.g. asthma, allergies, ADHD, and autism) should be required prior to any vaccine approval. Philosophical exemption, by which a parent can opt to delay or exempt certain vaccines for the child without discrimination such as loss of federal benefits or access to public schools, should be a fundamental right in the USA (as it is in Canada and other countries).
Clearly, the message hasn’t gotten through to SafeMinds, although perhaps I shouldn’t be surprised about that, given how research ethics appears not to concern anti-vaccine groups very much when it comes to their own, which is in marked contrast to their attacks on pharma and “conventional” science. Performing randomized, double-blind, placebo-controlled studies of currently used vaccines is completely unethical because it leaves the control group unprotected against vaccine-preventable disease. In fact, the only time such a trial could be ethical is if there is no currently existing vaccine for the disease; i.e., the vaccine is a new vaccine for a condition for which there currently isn’t a vaccine. If the vaccine is for a condition for which a vaccine currently exists, then the appropriate design of a clinical trial is to test the new vaccine against the old vaccine; doing otherwise would leave the control group unprotected against a vaccine-preventable disease. In addition, even doing epidemiological studies looking at health outcomes in vaccinated versus unvaccinated children is highly problematic, both on practical, scientific, and ethical grounds. On the other hand, in a perverse way, I’m glad that SafeMinds has put itself on the record as supporting an unethical clinical trial design motivated by its anti-vaccine views. It makes it so easy for me to go after its position.
The rest of its position is the same sort of superficially plausible-sounding nonsense that we’re accustomed to hearing from SafeMinds and its ilk. The real reason it wants access to data on vaccine injuries is so that it can “reanalyze” it and come to different conclusions, the way Mark and David Geier tried to do several years ago, and, of course, its call for “philosophical exemption” is nothing more than warmed-over “health freedom” rhetoric. Overall, then, there appears to be nothing new in the “philosophy” behind SmartVax. It’s nothing more than what we’ve been hearing from the anti-vaccine movement for a long time. It is, however, wrapped up in an appealing-sounding package. Unfortunately, the material is rotten to the core, just as pillar two of the SmartVax philosophy is unethical to its very core.
Where’s the beef?
Now that I’ve dealt with the revisionist history and Orwellian language of the “philosophy” section of the SmartVax website, let’s look at the “beef,” so to speak. What, exactly, is it that SafeMinds says about its “SmartVax” philosophy and what science does it use? The answer to the first question is, in essence, to claim that SafeMinds advocates “rigorous science” to justify its warmed over “too many too soon” complain coupled with an even more warmed over Bob Sears-style “alternative vaccine schedule” that would leave children unprotected against diseases like measles and pertussis for far too long. Perhaps the best example of the scientifically bankrupt and deceptive “SmartVax” reasoning can be found in a section entitled Weigh the Risks of Vaccination. One thing that is very apparent upon trying to wade through this site is that it superficially looks very “science-y.” However, the more I waded in, the more frustrated I became. In many cases, I couldn’t figure out how SafeMinds calculated its numbers and, worse, in many cases references weren’t easily locatable because they weren’t cited properly. For example, SafeMinds takes huge leaps based on a study of asthma rates in children in Manitoba based on vaccination timing but doesn’t actually cite the study on the page where it makes the claim or on the page where it explains the claim. This is a perfect lead-in to an example of the intellectual bankruptcy that is the SmartVax website.
Let’s take a look at the sorts of methodologies that SafeMinds recommends for estimating the “risks” of vaccination. Before I do this, however, let me just reiterate that it is a strawman argument that is being attacked when it is claimed that the “MaxVax” philosophy denies the possibility of vaccine injury. Scientists most definitely do not; in fact, it is scientists and physicians who study vaccine injury and estimate the frequency with which it happens, as well as potential predisposing factors. Think of it this way. Who did the studies that SafeMinds cherry picks? Not The difference is that scientists and science-based physicians base their estimates on science and epidemiology, not anecdotes, and most especially not on cherry-picked studies. Perhaps the most egregious example occurs when SafeMinds attributes a risk of 1 in 13 of “vaccine-induced asthma.”is administered according to schedule compared to a delay of three months, which leads it to produce this meaningless table. I also note that the Manitoba study was not a study of whether vaccination itself was associated with the later development of asthma but rather a study of whether the timing of vaccination with DPT was associated with asthma. There is a difference; yet SafeMinds uses the data from that study to make an estimate that 7.9% of the population is at a risk of “vaccine-induced” asthma from the DTP and Hib vaccines, even though the actual experimental group still got the vaccines, just three months later. One also notes that whole cell pertussis, as in the DTP vaccine, is no longer used in most countries. In any case, the authors themselves stated in the discussion:
On the other hand, McKeever et al did not find an association between asthma onset and the age at first injection of diptheria, polio, pertussis, and tetanus vaccine in their database of study of 29,000 children. To our knowledge we are the first to report that delay in adminstration of the first dose of DPT immunization is significantly associated with reduced risk of developing asthma in childhood.
One wonders why SafeMinds didn’t acknowledge this. It also fails to acknowledge that in the CDC study it also cites as evidence that the Hib and hepatitis B vaccines were associated with a weakly increased risk of asthma the relative risks were very low and the authors themselves did an analysis to determine whether a confounding factor might account for the elevated relative risk and concluded:
To evaluate the magnitude of possible medical care utilization bias, we performed a subanalysis restricted to children whom we knew were using two of the VSD HMOs (GHC and NCK) for their health care because they had made at least two medical care visits during their first year of life. In this subanalysis the relative risks for almost all of the vaccines of interest decreased, including those for Hib and hepatitis B. In another subanalysis in which we tried to reduce possi- ble health care utilization bias by restricting the analysis to children who had received at least two OPV, two DTP and one MMR, the relative risk of asthma associated with hepatitis B vaccine was less than that found in the main analysis. We conclude from these findings that the results of our main analysis are probably biased upward and tend to overestimate the relative risks associated with vaccination.
In conclusion medical care utilization bias did seem to influence the results for Hib and hepatitis B vac- cines, for which we found weak associations with asthma. Despite a similar bias that would favor finding an increased risk, we found that DTP, OPV and MMR vaccines did not increase a child’s risk of developing asthma.
In other words, the CDC Vaccine Safety Datalink team found no increased risk of asthma associated with vaccines for most vaccines, and for the two where they did the risk appeared to be very small and likely attributable to confounding factors. Yet SafeMinds mentions none of this, nor does it mention a recent meta-analysis that asks the question, “Is Childhood Vaccination Associated With Asthma?” The answer, in case you’re wondering, is a resounding no. Several other studies also support this conclusion, for example with respect to vaccination against pertussis and a recent German study that demonstrate no differences in allergic diseases between vaccinated and unvaccinated children. I will be honest here; the question of whether any vaccines are associated with an increased risk of asthma is not an entirely settled question yet, but one thing we can say. The vast majority of studies do not support such a link, and the Manitoba study is an outlier that needs to be confirmed, particularly given that it disagrees with a previous study. Moreover, the Manitoba study looked at a vaccine that is no longer used because its problems were recognized—by scientists!—and a safer version of the vaccine developed. Yet SafeMinds deceptively handwaves and in essence extrapolates a risk from a single outlier study to a more general risk and exaggerates a possible risk found in an old CDC study.
Such deceptive or incompetent (take your pick) biased cherry picking does not give me confidence in the rest of the “scientific” analyses of vaccine risks presented on the SmartVax website. Perhaps if I have time for a future post doing so, I’ll delve into the even more science-y tables presented as overall risks of vaccination versus the diseases protected against, but this post is already reaching a long length, and I’m getting tired. Also, I don’t want to finish without mentioning one last aspect of the SmartVax website.
Promoting anti-vaccine advocacy
Perhaps the most telling part of the SmartVax website is the About Us section. It’s all very confused, starting out focusing on mercury in vaccines as a cause of autism, even though it’s clear from numerous epidemiological studies that it almost certainly is not. It also parrots a number of anti-vaccine tropes:
Vaccines contain a number of components that have been linked to vaccine-injury, including aluminum adjuvants, mercury, antigens, and endotoxins. Research indicates that combining multiple vaccines into a combination vaccine can increase adverse reactions from vaccines, and also that adminstration of vaccines at an earlier age can increase risk of vaccine-injury. Research has not been performed on most vaccines in vaccinated vs unvaccinated children to determine whether there are links to the autism, ADHD, and allergy epidemics; research on asthma indicates that there is a link to vaccines. The entire USA vaccination schedule, which has approximately tripled since the 1986 law which protects manufacturers from vaccine lawsuits, needs to be studied and analyzed with an unbiased approach to find scientific answers. Similarly, there is a dearth of research on “Environmental X Factors” that contribute to these epidemics.
Yes, indeed. It’s the “toxin gambit,” coupled with “too many too soon” and the myth of an “autism epidemic” all rolled into one. SafeMinds then goes on to say:
Beyond the personal impact to individuals and families, the epidemic of vaccine-injuries has enormous implications to the public. A future America will be competitively disadvantaged due to medical costs, lost wages, reallocation of personnel into care-giving roles, and a smaller pool of qualified military recruits. Such a bleak future can be avoided, but it will require the American public to take action. Synergistic research from diverse scientific fields such as toxicology, endocrinology, and immunology could lead to a fundamentally new scientific understanding of how vaccines work and how vaccine injuries occur. This could provide the knowledge of how to design a new vaccination program that is both safer and more effective. But recent history indicates that Max-Vax proponents in the government and public health industry will suppress such science, unless there is a “SmartVax” consumer advocacy movement to protect these researchers from discrimination and encourage elected officials to insist that the CDC and FDA take action to recognize and reduce vaccine-injuries.
At its essence, the SmartVax philosophy is all about being smart with vaccinations: don’t over-use them, pursue the science, understand the risks, and ensure that the risks are not hidden from the public. A SmartVax approach will lead to improved children’s health by minimizing vaccine-injuries and protecting against infectious diseases. With SmartVax, the future vaccine program will be both safer and more-effective.
Except that, as I have just shown, SmartVax isn’t so smart about pursuing the science. The purported link between vaccines and asthma is but one example. In every case I’ve taken a look at, SafeMinds has cherry picked data, choosing only the research that suggests the highest risk and discounting all the other research that finds no risks. In the rest, SafeMinds distorts history, uses logical fallacies, and in general does its best to hide its anti-vaccine agenda. Amusingly, that is not enough. Looking through the comments of the announcement of the SmartVax site on AoA, I find it apparent that anti-vaccine advocates are not happy, nor are they necessarily fooled. Here are some examples:
I’m anti-vaccine as well because I have seen first hand the effects of vaccines especially the MMR and in your case the DPT. Vijendra Singh noted that in his studies but of course the pro-vaccine lobby ignored his studies and focused their attacks on Andy Wakefield. The moderates in the community are basically kissing up to the pro-vaccine lobby. The moderates are timid and don’t support families and kids, unfortunately by their timid behavior.
None of us can change this behavior because these people are afraid of their own shadows. So families and kids will continue to suffer because of this cowardly behavior….on the part of parents/organizations.
Shameful. We can expect it from vaccine companies….but can we expect it from parents and autism/vaccine organizations????
Apparently so!!!
Next, here’s someone by the pseudonym veritas:
I agree with Elizabeth. Only no vax guarantees the total safety. All pediatric infectious diseases are trivial at our time, as can be treated or managed with antibiotics or proper care. I would not risk my child life with any vaccine now. They become more and more toxic and we have no idea what is in them. Experience of EU, where only a small fraction of parents vaccinate, is the best evidence that mass vaccinations are not needed and harmful. More children now die from vaccines than from infectious diseases; although tens of thousands vaccinated or not get sick from infectious diseases, they very rarely die in developed coutnries. The reverse is true with vaccines. You can recover from infectious diseases, but it is very difficult to recover to recover from vaccine-induced injuries, such as diabetes, asthma, chronic encephalopathy, autism, etc.
Actually, let’s look at the experience of the EU, where measles has returned with a vengeance, all thanks to a large pool of unvaccinated children. As for verities’ comment about all pediatric infectious diseases being “trivial” at our time, I would remind this ignorant person that, yes, even in 2011 children die of pertussis in the United States. Children still get hepatitis B and later develop cirrhosis or liver cancer at a young age. In 2011. This doesn’t even take into account the morbidity and suffering that many vaccine-preventable childhood diseases can cause.
Truly, veritas has chosen poorly for his pseudonym, given the misinformation he or she is peddling.
To conclude this post, here’s Kathy Blanco, whom I quote in her entirety:
Here we go again, the spineless approach to this worldwide epidemic, yeah, let’s be politically correct now? Not. Although I appreciate the EFFORT, to appear non aluminum foiled hatted, I know without a shadow of doubt, that it is and can trigger autism in our children. I believe NO vaccine has value or efficacy and so do top experts who have any job left. Perhaps when they read the site they may as in BIG may come to that conclusion. However, I have come to the further conclusion, that as not only a recipient of a damaging vaccine in my children (which sways opinion/vested interest, no lying), but, that the science does not support they are safe in any way, shape or fashion. That means the crowd that ashews no mercury, etc, are in fact, half right and half wrong. And I am afraid the mixed message of compliance, we can work with you attitude, is like saying, a murderer can get off or out of jail after good behavior. These people KNEW it was causing damage, and there is the bigger item for interests, and to be frank…the average parent gets the narly vision of a double breasted suit wearing liar in a vaccine regulatory chair/aka dollar signs, rather than explaining by statistic how this or that would cause or MAY cause something in their child. I think people sense the lying on pharma adds, and see the double standard business as usual stance on vaccines. Since we have started this “workable” parent routine, more vaccines have been added to the schedule. Do you know what they really don’t want to happen? Take a guess, it’s called the pocketbook. It’s called a general boycott, furthering exemptions or keeping them. That’s what they listen to. Not our sad puppy eyes, signs of damaged children at a march. Not even lawyers get them going. They know they are protected from damage claims even by the highest levels of our government, and they will continue their carnage until we finally get it, or they have completed their mission of the “soft kill”. The reality is…we are the consumers, and not consuming their garbage will stop their lying son of a gun asses. Sorry, thats this mommies humble wordly view of it. I tried to many years ago, to illuminate what child would become autistic if given a vaccine, just like this website, however, I had the balls to say it, no vaccine is safe, and don’t experiment on YOUR child. I know this won’t go pass the moderator, but it makes me feel better just typing it. What I was doing however, was suggesting to an unknowledgable average citizen, is that vaccines represent an immune challenge for which our children, in general can not handle, even on it’s premise, is the fact it is never tested in immune damaged children. And how can one “determine” such…it is more than autoimmunity in the mother, a a whole HOST of factors, generally felt by all in our community at large (toxic poisoning of our bodies by industry), that is WIDELY felt. No one goes unscathed. So therefore, no vaccine is safe. None. Deleyed reactions, of course, it’s called oncogenicicity (cancer forming), or to put it more mildly, chronic immune activation, and more mildly, WITCHES BREW.
In the end, SafeMinds is fooling no one. Its protestations otherwise that it is not “anti-vaccine” do not fool those of us who know better. Its torturing of the science, liberal use of revisionist history and bad arguments, and its favoring of Orwellian language, all coupled with never, ever conceding that any vaccine is safe and effective and never, ever accepting the evidence consistent with vaccines having no etiological role in autism pathogenesis, speak much louder than any “SmartVax” website. Even more amusingly, SafeMinds’ attempts to paint itself as a “pro-safe vaccine” organization appear to be backfiring spectacularly among the real anti-vaccine underground. Perhaps SafeMinds would do better to let the mask drop and let its anti-vaccine freak flag fly. However, if it ever did so it would lose any tiny bit of credibility that it can snooker the press into giving it. Consequently, SafeMinds’ attempts at twisting science and language will likely continue, as it walks the tightrope between disillusioning its anti-vaccine base and making it undeniably clear to everyone what a crank organization it is.
In a way, I almost feel sorry for SafeMinds. Well, not really.
![]()
![]()
![]() <!--<!--
<!--<!--![]()
![]()
![]()
![]()
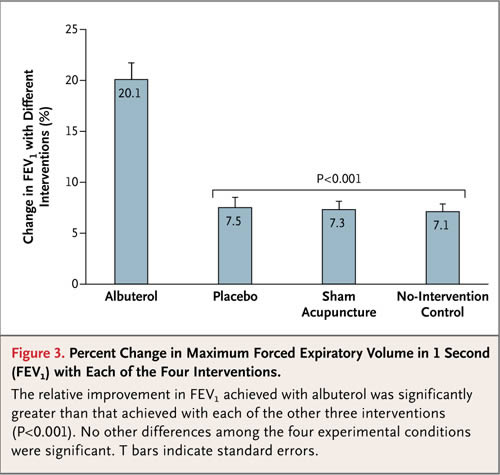
 We understand that asthma is not just a tightening of the airways but also an inflammation that can cause long-term damage. Not only can we treat asthma, but we have objective ways of measuring how well our patients are doing. It’s easy and inexpensive to measure airway obstruction and response to medications. We know what works.
We understand that asthma is not just a tightening of the airways but also an inflammation that can cause long-term damage. Not only can we treat asthma, but we have objective ways of measuring how well our patients are doing. It’s easy and inexpensive to measure airway obstruction and response to medications. We know what works.






![[Diagram]](http://www.sciencebasedmedicine.org/wp-content/uploads/2011/07/pic2.jpg)
 The picture above shows the clumping of the cells. Immediately it seems as if there can be a problem applying this to a person. The glass tube used in the study was larger than the smallest arteries in people. Further, capillaries are only large enough to allow red cells to flow through single file. I would not want my red cells clumping as in the picture above and then trying to squeeze through capillaries. I would not be surprised if the effect on viscosity were reversed for smaller arteries, or even caused serious problems with capillary flow. But I suspect the net effect on blood flow in vivo is negligible, because we have been exposing people to magnetic fields of this strength in MRI scans for a couple decades now without any ill effects.
The picture above shows the clumping of the cells. Immediately it seems as if there can be a problem applying this to a person. The glass tube used in the study was larger than the smallest arteries in people. Further, capillaries are only large enough to allow red cells to flow through single file. I would not want my red cells clumping as in the picture above and then trying to squeeze through capillaries. I would not be surprised if the effect on viscosity were reversed for smaller arteries, or even caused serious problems with capillary flow. But I suspect the net effect on blood flow in vivo is negligible, because we have been exposing people to magnetic fields of this strength in MRI scans for a couple decades now without any ill effects.