
Ok living in a city of 18 million people not far from China you would think there would be a big vibrant China town. I had heard two versions one it was great but from a guy on the course who lives here I was told not to bother. Ignoring him I head off there Friday evening and let me tell you it was a great disappointment. Now before I go to far it may be my fault maybe I missed the nice par
Monthly Archives: September 2011
U S A
No I am not coming home yet but a slice of home came here this past weekend for the Rugby World Cup. Thats right the United States Eagles our very own Rugby team which I did not know we had until this trip came to Wellington to take on the Australians. Of course being Americans in New Zealand we had to support our country no matter how bad our team is if your unfamiliar with rugby we are awful
Additonal Info
Sorry folks. For some reason my last blog dropped off a few sentences at the end so I39ve added this bit so that it makes sense.I think the end of the blog 39Three Days to Go39 said something about how I had added some family and friends email addresses to a list that should get an automatic email notification whenever we post of new blog. To test how this works could you please send us
1 Month In
Just over 1 month in and Im over the culture shock which was surprisingly worse than I imagined it would be. I think 3 months back in England and I had reverted back into the comfort zone as well as missing my life and friends in South America. Te extrano chicos But pastures new...Ive started work and am discovering what it is like to teach classes of shy reserved Vietnamese adults
My Rugby World Cup Part I
When the IRB announced in 2005 that New Zealand would be hosting the 2011 Rugby World Cup I vowed I would go. Since my high school exchange here I have made the pilgrimage to my second home twice before. My fourth visit to New Zealand is technically my fourth and fifth visits since I39m punctuating my time here with a trip to Australia.My Rugby World Cup experience began on September 11 wh
Society Discrimination
1. The article India 39s Untouchables Face Violence Discrimination relates to the concept we are currently exploring in class because it demonstrates how the Dalits untouchables are still present in India and also states how they are the lowest social class who suffered severally and treated as if there less than humans. Also Hindus is very determined to keep this progress going. 2. B
A Vacation in Maine
Ah...a real vacation It had been about 5 years since Id been on a real vacation...you know one that takes you out of the state that you live in. For the past 5 years my breaks were spent in Vermont. Ive always enjoyed all of the activities that Vermont has to offer for each season of the year. Its always kept me busy and happily entertained. The main purpose for the trip was to see
RIHLA 3
1 This relates to what we are learning in class because we are learning about how people were treated differently because of their social class. Also in the article it talks about how people are treated different becasue of how much money is made by them.2During class in the Hinduism and Caste system stimulation I think everybody played their part well. I think so because you could see how every
Road To Rukwa Day 7
We slept in knowing there was nowhere to go and nothing to do for the day.We are staying at a Catholic Retreat Centre run by the Benedictine monks. The land is sparse but it sits right on the shore of Lake Tangayeka. The rooms are primitive to say the least. I had a shower that doesnt work so bucket showers were in order. This is where you fill a bucket with cold water pour it over you
Last days at Wonderland Incheon and first days at Kid’s College Gangseogu Seoul.
Wow so it turns out I wasRUBBISH at keeping this blog up to date. I say 39was39 because I intend to correct that.Last thing you heard from me I was still in my 1st year in Korea and loving every second well things didn39t change much. My contract came to its natural end at Wonderland School in Mansudong quiet a challange for most people in Korea who get sacked just before the end of
Journey of a Lifetime
Hi EverybodyThe TransSiberian is the journey of a lifetime and an epic trip into some of the worlds most remote landscapes through spruce and birch forests traditional villages and endless steppes. The trip across Russia is one of the longest railway journeys in the world starting in Moscow and ending in Vladivostok. Walt and I are not going the entire 6000 miles to Vladivostok the P
Arriving at Las Vegas
at about 8.30 at night we arrived in a sea of light at the city of las Vegas. A beautiful sight all those lights. No carbon tax here. Everything went smoothly so within half an hour we were outside a cool airport into a warm Nevada night. A cab took us quickly to our Monte Carlo hotel. The check in gave us a nice room on the 27th floor that gave a nice view over part of the city. On those small fl
Arkansas
Hi all well it is not long now before I will be heading home and looking forward to Aotearoa. Alot has happened since we last blogged mostly unexpected events. We left Washington DC and headed too Chicago to catch a connecting flight to Memphis only to find that our flight had been cancelled and the next one won39t be until the following day all good. They just put everyone up in a hotel with
Three Days to Go
Well it is now only 3 days before we leave on our big trip and everyone is telling us nthat we must be excited. However we are both still very busy with everything else at the moment and with two or three days of work left we are still trying not to focus on the trip too much Yeah right I hear some of you saying.Everything is ready as far as we know and it is now just a matter of making sure
Pictures tell a thousand words..
Not many words today just some photos to back up my recent ramblings....hope you39re all enjoying your Sunday. Today is my first day off in ages so I just went for a long walk didn39t get lost woohoo and checked out my neighbourhood. There is a food market in the next street and all I can say is that if our cook gets her meat there I39m turning vegetarian I39ve seen plenty
Recycle
Like most people who grew up after April 22, 1970, I think it is important to be as environmentally responsible as possible. Like many I fail miserably much of the time, but at least I feel guilty about it. Recycling offers the opportunity to feel good about my environmental impact with little effort, since the garbage collection infrastructure in Portland makes recycling easy.
Some products are best extensively reprocessed before reused. Urine, as an example. There are proponents of topical and/or drinking urine as a treatment/cure for nearly any illnesses. The kidneys are mostly responsible for fluid and electrolyte balance and I realize that normal urine is mostly water, salts, urea and a smattering of other very dilute molecules. I have the urine tox screen to prove it. Urine is not a particularly noxious body fluid, but it is not high on my list of liquids to drink under normal circumstances.
Urine is mostly water but not an optimal source of water if it is your only source for fluids. Urine drinkers love to mention the occasional trapped earthquake victim who survives, in part, from drinking their own urine. For the first several days the urine would be dilute enough to keep people reasonably hydrated, as humans cannot concentrate urine as well as, say, a camel. So I can see where consuming urine for a short period of time would delay progressive dehydration and death. A couple days of drinking urine neat, shaken not stirred, would be harmless and, if there were no alternative sources of water, beneficial. I do suffer from the societal taboo that piss is icky, and for aesthetic reasons urine is not something I would want to consume, even when it is referred to as its more common designation ‘Coors Light’.The kidney, I should mention, is the only organ in the body that functions on magic. Really. Does anyone actually believe/understand the function of the so called Loop of Henle? I scoff at those who talk about human energy fields or water having memory, but as best I can tell, the Loop of Henle is no different. My undergrad degree was in physics, so at some point I suppose I ‘understood’ quantum mechanics and relativity, at least well enough for the tests. The Loop? Bah. Total smoke and mirrors.
Drinking your own piss has a long history, especially in India and Asia and advocates (mis)quote the bible:
Proverbs 5:15. Drink water from your own cistern, running water from your own well.
Although the following verses suggest that it is a metaphor for marital fidelity, not consuming pee. The bible has never been a convincing source of medical advice, although with teenage boys at home, I increasingly see the wisdom of Deuteronomy 21:18-21, Exodus 21:17 and Proverbs 30:17.
The rationale behind drinking your urine is simple: it is an ultrafiltrate of all that is best in the blood, with none of the toxins, which are processed and disposed of by the liver. So when you drink your urine, you are consuming a golden elixir of salts, proteins, and hormones, containing all you need to treat virtually every disease and maintain health. Sort of an uber-energy drink with none of the caffeine and fewer calories. Your own, early morning, midstream urine is to be preferred, and in a pinch you could drink others urine, preferably from the same sex. I suppose it would be wise to avoid the urine of the autistic, it being loaded with mercury, aluminum, and perhaps other toxic metals.
Are there uses for urine? Popular culture has it that peeing on a jellyfish sting will relieve the pain; this is neither supported or denied by the Pubmeds. It appears to be the one therapy with no supporting Cochrane review. Urine on a jellyfish sting, if dilute, is counterproductive, since fresh water will trigger jellyfish nematocysts to fire and increase the pain of the sting.
Similarly, topical urine is advised for bee, mosquito and other venomous bites, with neither supporting or disconfirming data. Given the medical benefits of urea (mostly as a moisturizer at concentrations many fold higher than in the urine) and other molecules in urine, they may be products in piss that would inactivate venomous stings. I can’t dismiss the concept out of hand, although concentrations in the urine of well hydrated people would be minimal. So use the urine from a trapped earthquake victim or lifeboat survivor, which will become concentrated with time, and not your Corona addled swimming or hiking partner.
It is an ongoing curiosity how proponents of curious therapies will take a bit of truth an magnify its significance out of all proportion to reality. An example.
Urokinase is a protein that has utility in dissolving clots. Its dose, depending on what is treated, is around 500,000 to 2 million units IV. Normal urine contains urokinase, but how much? ” Normal human urine contained 2068 ± 0.36 u/ml of UK” Hardly enough to have any effects should it be consumed orally, especially given the ability to the gi tract to reduce any protein to amino acids. Yet because urokinase is useful in high doses iv in patients with clot, it is also useful orally as a medicine. Odd logic.
One site notes there are 2 grams of protein and a 100 mg of glucose excreted the urine a day. Is that lot? A dollar bill weighs a gram and we make 1 to 2 liters of urine a day. So a cup of urine will contain about half a dollar bill in weight of protein (roughly the same as a McDonalds meat patty) and 25 milligrams of glucose, about as much as the “one” on the back of a dollar. Compare that to 8,000 milligrams of protein and 12,000 milligrams of glucose in a cup of milk. Not quite homeopathic concentrations, but close.
The arguments behind the use of medicinal piss are the usual: appeals to antiquity (not mentioning the average life expectancy of the ancients was just a tich longer than a fruit flies), innumerable anecdotes, and the ever popular secrets “they” don’t want you to know.
The medical community has already been aware of [urine's] astounding efficacy for decades, and yet none of us has ever been told about it. Why? Maybe they think it’s too controversial. Or maybe, more accurately, there wasn’t any monetary reward for telling people what scientists know about one of the most extraordinary natural healing elements in the world.”
It is getting increasingly difficult to keep track of all the miracle cures I am supposed to keep secret. One of these days I am going to slip up and inadvertently cure someone with an effective and inexpensive natural remedy. Even dogs and monkeys participate in the healing effects of drinking their own urine. Or they have sloppy aim. Of course monkeys and dogs eat their own vomit, so I doubt they have a discerning palate.
My Loop of Henle psychosis not withstanding, the understanding of renal physiology by urinologists is, well, interesting. One site calls urine “purer than distilled water” and then lists all the beneficial chemicals in the urine. Given that the purpose of distilled water is to make the product nothing but H20, it is an interesting contradiction.
or
Urine is believed to be a byproduct of blood filtration. It is NOT excess water that is released by the body. When blood filled with nutrients pass through the liver, the toxins are filtered out and are excreted as solid waste. The purified blood then travels to the kidney where excess nutrients are eliminated from the body.
George Carlin used to talk about ‘jumbo shrimp’ and ‘military intelligence’; perhaps we should add ‘CAM understanding’ to the list.
The problem is getting the nerve to drink your piss since there is an aversion to consuming pee. As Rita Mae Brown said in a different context, “Nothing is unnatural – just untried.” If you work yourself up to it, all things are possible:
How many people do you know who have drunk enough urine to really know what it tastes like? Probably not too many. Those who regularly drink their own urine say it. But taking urine into your mouth might be too big a step to begin with. Rubbing a drop into the and first smelling your own urine can help you to overcome part of the barrier. Really, it often does not smell bad at all. Many people even like its sometimes sweet odor. More extensive massaging of urine into your skin is also a good way to become accustomed to your life water. How can you overcome feelings of aversion to drinking your own golden elixir? Start by drinking a drop then a sip each day and slowly build up to a fill glass of urine. This is the most comfortable way to allow your body, mind and soul to become accustomed to this therapy.
I’ll pass.
It would seem for those who participate in urine therapy there is a certain embarrassment in talking about their life changing cure for everything. It is kind of sad, really, and I feel for them. It must be difficult to have easy access to the cure for all diseases and have to feel uncomfortable about discussing it due to societal taboos. And if we meet in public, really, I don’t want to know if you drink piss. That would be, under almost every circumstance, the OED definition of over-sharing.
Urine therapy is, of course, a panacea.
…one of the most powerful, most researched and most medically proven natural cures ever discovered. Multiple sclerosis, colitis, lupus, rheumatoid arthritis, cancer, hepatitis, hyperactivity, pancreatic insufficiency, psoriasis, eczema, diabetes, herpes, mononucleosis, adrenal failure, allergies and so many other ailments have been relieved through use of this therapy
Not a bad list. Looking on the interwebs, there is no medical condition that is not amenable to treatment with either topical or oral urine, and they wisely advise against intravenous injection.
Any evidence for efficacy? Nope. Just testimonials.
Any reason to suspect drinking your piss would help any medical condition? No. Given the dilute nature of the products in urine, it should be neither helpful nor harmful.
Of course, the lack of efficacy or plausibility is no hindrance to use. As one web site on the mechanism of urine therapy notes
…theories have never been proven using modern scientific procedures to verify his ideas, and at some levels has been completely dis-proven, but nevertheless people still believe them. Maybe the power of belief in this instance overcomes what factually may not be real.
Sums up the whole field of alt med, does it not?
Addendum
The links to sources in this entry may or may not refer back to original sources. As is often the case in the more marginal CAM therapies, many sites appear nearly identical in content, one large cut and paste fest. Even Vanderbilt University regurgitates the same text as if were original without proper references; one would think a University would be sensitive to issues of plagiarism, although perhaps Vanderbilt is the original source.
![]()
![]()
![]() <!--<!--
<!--<!--![]()
![]()
![]()
![]()
Legislative Alchemy II: Chiropractic
As we learned in Legislative Alchemy I: Naturopathy, legislative alchemy is the process used by state legislatures to transform implausible and unproven diagnostic methods and treatments into legal health care practices.
Today, we review how chiropractors are faring in the 2011 state legislative sessions.
Chiropractic 101
In 1895, a self-described “magnetic healer,” Daniel David Palmer, claimed to have discovered that every person possessed an “Innate Intelligence,” defined as the body’s capacity to heal itself, which flowed from the brain out through the nerves in the spinal cord. Misaligned vertebrae impinged on nerves and interfered with the flow of Innate Intelligence, causing “95 percent of all disease.”
Palmer named these putative misalignments “subluxations,” and began teaching students how to detect and correct them based on his notion that removing this interference would return the free flow of Innate Intelligence and the body would heal itself. In other words, chiropractic was — and, as we shall see, still is — simply another form of vitalism, a long-discredited notion that illnesses are caused by a disturbance or imbalance of the body’s “vital force,” which is distinct from the body’s biochemical processes.
Palmer and his disciples were arrested for practicing medicine without a license, which led to a strategy of chiropractors lobbying state legislatures for their own chiropractic practice acts. This effort stretched from 1913, when Kansas became the first state to license chiropractors, to 1974, when Louisiana became the last.
Subluxation: it’s the law
The non-existent chiropractic subluxation remains the central tenet of the 50 state chiropractic practice acts to this day.[1]
Twenty-one state chiropractic acts mention it specifically as the basis for chiropractic practice. For example, Connecticut defines chiropractic practice as:
the science of adjustment, manipulation and treatment of the human body in which vertebral subluxations and other malpositioned articulations and structures that may interfere with the normal generation, transmission and expression of nerve impulse between the brain, organs and tissue cells of the body, which may be a cause of the disease, are adjusted, manipulated or treated.
Twenty-three states refer to its purported attributes — without actually using the “s” word. In North Carolina, chiropractic practice is defined as:
the science of adjusting the cause of the disease by realigning the spine, releasing pressure on nerves radiating from the spine to all parts of the body, and allowing the nerves to carry their full quota of health current (nerve energy) from the brain to all parts of the body.
Did they say “science”? Here’s how much science is involved in chiropractic’s core concept — there’s not even a plausible hypothesis of what a subluxation is or how it might affect human functioning.
Six states simply incorporate by reference practices and procedures taught in chiropractic schools, which remain loyal to the subluxation although some have tried to distance themselves from the word, if not the concept.
This doesn’t mean, of course, that chiropractors are permitted by law to treat any disease or condition by detecting and correcting subluxations, just most any disease or condition, as long as the problem is defined in terms of the patient’s having one or more subluxations stopping up the “flow” of “nerve energy.” Asthma, allergies, ADHD, painful periods and earaches are a few of the many conditions widely advertised as treatable by chiropractic adjustment.
You might think it would cause the chiropractic industry some alarm that legislators might wake up to the fact that subluxations don’t exist. And apparently that is the case. In a few states chiropractors are attempting to expand the chiropractic scope of practice by including authority to prescribe that former anathema to chiropractic: drugs. For years chiropractors branded themselves as doctors who treat patients “without drugs or surgery.”
With drugs but not surgery
Chiropractic lobbying in New Mexico, the state where anyone can practice medicine, provides a perfect lesson in the insidious nature of CAM practitioner licensing. A few years ago, the state legislature invented a new iteration of chiropractor, the “certified advanced practice chiropractic physician.” With minimal training, this new type can, by statute, “prescribe, administer and dispense herbal medicines, homeopathic medicine, over-the-counter drugs, vitamins, minerals, enzymes, glandular products, protomorphogens, live cell products, gerovital, amino acids, dietary supplements, foods for special dietary use, bioidentical hormones, sterile water, sterile saline, sarapin or its generic, caffeine, procaine, oxygen , epinephrine and vapocoolants.”
Then, in 2009, the New Mexico legislature granted the state chiropractic board authority to develop a formulary for the “advanced practice chiropractic physician.” The requirement that substances be “natural or naturally derived” was eliminated, but there was a catch: “Dangerous drugs or controlled substances, drugs for administration by injection and substances not listed [in the quoted section, above] shall be submitted to the board of pharmacy and the New Mexico medical board for approval.”
Apparently, approval was not forthcoming to the chiropractors’ satisfaction, so they returned to the New Mexico legislature this year, seeking to dump the pharmacists and medical doctors. A new, improved version of the “advanced practice chiropractic physician” was proposed: one with a “prescription certificate.”
And just to make the point clear, the term “chiropractic” would be discarded from the New Mexico chiropractic practice act in favor of “chiropractic medicine.” Thus, the purpose of the practice act went from “granting chiropractors the right to practice chiropractic as taught and practiced in standard colleges of chiropractic” to granting “chiropractic physicians the right to practice chiropractic medicine …” [Emphasis added.]
Gone was the requirement of a pharmacy and medical board approved formulary. Instead, those with the “prescription certificate” would be authorized by statute to “prescribe, administer and dispense dangerous drugs, including compounded preparations for topical and oral administration and injection, testosterone in all its forms and codeine in cough syrup.” [Emphasis added.]
One can read between the lines thinking that goes something like: “If the pharmacists and medical doctors won’t let us prescribe testosterone ‘in all its forms’ and cough syrup with codeine, we’ll just put it in the statute and they can’t do a damn thing about it.”
Instead of pharmacy and medical board approval, the proposed legislation provided that “the [chiropractic] board, with the New Mexico Medical Board and the Board of Pharmacy serving in an advisory capacity, and with all parties agreeing to act in good faith, shall establish by rule a formulary …” [Emphasis added.]
Yeah! That’ll show ‘em!
Except the proposed legislation didn’t pass. It was still in committee when the legislature adjourned. New Mexico’s governor recently declared a special session of the legislature to deal with certain pressing problems, such as redistricting, and that has begun. We can only hope the chiropractors don’t try to shoehorn their bill into the special session agenda.
As a cautionary tale about the dangers of mission creep in “CAM” practitioner licensing, it is instructive to look at the education and training which would have been required of the “certified advanced practice chiropractic physician” in obtaining a “prescription certificate.”
In addition to the minimal requirements for “advanced practice” certification, the applicant must complete “pharmacological training from an institution of higher education approved by the [chiropractic] board or from a provider of continuing education approved by the board.” [Emphasis added.]
The applicant must complete a program, again approved by the chiropractic board, of 200 classroom hours in pharmacology, physiology, pathophysiology, physical and lab assessment and clinical pharmacotherapeutics, which, you’ll have to admit, is a really long word. Whether this is simply descriptive of, or in addition to, the education described in the previous paragraph is not clear. What is clear is that all of this can be accomplished within the current chiropractic educational system, a subject to which we will return in a future post.
But where, you might ask, would the chiropractor get experience actually treating patients with drugs, so essential to proper training? Well, remember those pesky medical doctors who were gumming up the formulary works? The ones the legislation sought to remove from the process? From them, that’s who.
In order to get the coveted “prescription certificate,” a chiropractor would have to complete 400 hours “of clinical rotation practicum in clinical assessment and pathophysiology” and 400 hours of 100 patients “with disorders relevant to the certified advanced practice chiropractic physician’s clinical specialty.” All done “under supervision of a medical doctor.”
One must wonder where one would find a medical doctor willing to take on supervision of a chiropractor treating patients with drugs.
A bad idea metastasizes
The chiropractic faction interested in foisting chiropractors as primary care physicians on the public was obviously not going to stop with New Mexico, and it didn’t.
In South Carolina, a bill would have created the same sort of “advanced practice chiropractic physician” as presently exists in New Mexico along with the option of obtaining a “prescription certificate” as proposed in the failed New Mexico legislation. The bill never made it out of the Senate Committee on Medical Affairs.
Likewise, in Alabama, a bill was introduced to allow prescription of “natural” compounds, “bio-identical hormones,” homeopathic remedies and other woo remedies favored by “CAM” practitioners. If the chiropractor took the same sort of 90-hour course as New Mexico allows, he or she could also prescribe and inject these substances even if they were classified as legend drugs. This bill also died in committee.
More scope of practice
Prescription authority was not the only means of increasing ways to make mon … I mean, increasing the scope of chiropractic practice attempted in this year’s legislative sessions.
In Illinois, lobbying efforts took a more subtle approach and attempted only an inclusion of authority to provide advice regarding the use of non-prescription products. Translation: they can advise patients regarding dietary supplements. And, of course, having given that advice, they can sell patients the supplements they’ve recommended. This bill, which also authorized chiropractors to administer atmospheric oxygen, made it into law. A bill in Hawaii, authorizing the use of “clinical nutritional methods” (whatever that means), died in committee.
Minnesota, another state where anyone can practice medicine, saw a failed attempt to include acupuncture within chiropractic scope of practice. Perhaps wary of attempts to make chiropractors actually go to acupuncture school and learn “real” acupuncture, this proposed legislation invented an entirely new form, defined as “a modality of treating abnormal physical conditions by stimulating various points of the body or interruption of the cutaneous integrity by needle insertion to secure a reflex relief of the symptoms by nerve stimulation as used as an adjunct to chiropractic adjustment.” Maybe they should have called it “acujustment”.
And on it goes
Last year, the Connecticut Board of Chiropractic Examiners issued a ruling that chiropractors need not warn patients of the risk of stroke following cervical manipulation, a ruling based largely on a study which specifically states it does not rule out such a risk.
In response, Connecticut Senator Len Fasano promised to introduce legislation in 2011 mandating a warning. Sen. Fasano testified at a hearing before the Board that he and others in the legislature were under the distinct impression the Board would indeed require this type of warning. Obviously, the Board did not do that, so Sen. Fasano kept his promise and introduced a bill requiring chiropractors to obtain informed written consent prior to any treatment of the cervical spine, including information on the risk of stroke. Unfortunately, the bill did not make it to the floor for a vote.
Finally, chiropractic lobbying in Florida screwed up passage of a perfectly good bill designed to protect the public’s health, safety and welfare.
A bill introduced to educate coaches, parents and young athletes about sports-related concussions and to require that an M.D. or D.O. sign off on return to play post-injury passed the House, where an attempt to include chiropractors was rebuffed in committee. However, the bill got bogged down in the Senate because of a similar attempt to force the inclusion of chiropractors in the type of health care practitioner with authority to clear the young athlete for continued play. The implication, of course, was that chiropractors were qualified to diagnose and treat traumatic brain injury, a conclusion not universally shared in the Senate, and rightly so. That squabble ran the clock out on what would have been a laudable safety measure for school athletes. And that’s a shame.
Conclusion
It is unfortunate enough that the state legislatures have legitimized a figment of the imagination first proposed by a charlatan in 1895 — the “subluxation” — by creating a licensed health care profession known as chiropractors to “detect” and “correct” them. Giving chiropractors authority to prescribe dietary supplements, and, even worse, drugs, only exacerbates their original mistake. Instead of expanding the scope of practice, state legislatures should remove diagnosis and treatment of the nonexistent “subluxation” from the chiropractic practice acts.
References
- Bellamy J., Legislative Alchemy: the US state chiropractic practice acts, Focus on Complementary and Alternative Therapies (2010)15(3): 214–222.
![]()
![]()
![]() <!--<!--
<!--<!--![]()
![]()
![]()
![]()
Some Encouraging Backlash Against Nonsense
One of the themes of SBM is that modern health care should be based upon solid scientific ground. Interventions should be based on a risk vs benefit analysis using the best available scientific evidence (clinical and basic science).
As an extension of this, the standard of care needs to be a science-based standard. Science is (or at least should be) objective and transparent, and without such standards there is no way to have meaningful quality control. Without the filter of science there is no limit to the nonsense and magical thinking that can flow into the health care system. Increasingly we cannot afford the waste of fanciful and ineffective interventions, and even if limited resources were not an issue – individual patients deserve better.
It is for these reasons that we oppose the attempts by proponents of so-called complementary and alternative medicine (CAM) to erode or eliminate the science-based standard of care in medicine. Proponents differ mostly on how open they are about this goal, but there is no escaping the reality that at the heart of the very concept of CAM is at least a double standard – one in which the science-based bar for inclusion is lowered for some favored modalities.
Proponents will sometimes argue (against all evidence) that this is not the case but rather that there is prejudice and closed-mindedness against certain types of treatments. This is reminiscent of the claims by proponents of creationism/intelligent design that their beliefs are unfairly treated by scientists and school systems. In fact both cultural movements use the same language and tactics to promote their ideology against the defenders of a science-based standard -the “academic freedom” and “health-care freedom” strategies are two sides of the same coin.
Our primary mechanism for opposing the weakening of the science-based standard in medicine is simply to point to the rhetoric and tactics of the CAM proponents themselves. While they largely operate below the radar, when the light is shone on what they are actually doing the “shruggie” masses sometimes take notice. This occurred recently in Ontario, and provides an excellent example of all that I described above.
The conflict is about the College of Physicians and Surgeons of Ontario’s (CPSO) draft guidelines on Non-Allopathic (Non-Conventional) Therapies in Medical Practice. The first clue that these guidelines are likely to be problematic is in the title – the word “allopathic” is only used by CAM proponents. The term was coined by Samuel Hahnemann, the inventor of homeopathy, to refer to the conventional medicine of his day – prior to the incorporation of scientific methods into medicine. It does not reflect the philosophy or practice of modern medicine, and it is a pejorative term.
The guidelines also assume that “non-conventional therapies” should be incorporated into medical practice. Shouldn’t that be the real question, rather than just assuming they should be then exploring how to do so? The only justification given (the most common one given) is popularity (a fallacy deconstructed numerous times on this blog).
But that aside, here are the recommendations for how “non-conventional” therapies should be incorporated into practice:
Physicians are expected to propose both allopathic and non-allopathic therapeutic options that are clinically indicated or appropriate.
Any non-allopathic therapeutic options that physicians propose to patients must:
- have a demonstrable and reasonable connection, supported by sound clinical judgement, to the diagnosis reached;
- possess a favourable risk/benefit ratio, based on the merits of the option, the potential interactions with other treatments the patient is receiving, and other considerations the physician deems relevant;
- take into account the patient’s socio-economic status when the cost will be borne by the patient directly; and
- have a reasonable expectation of remedying or alleviating the patient’s health condition or symptoms.Reasonable expectations of efficacy must be supported by sound evidence. The type of evidence required will depend on the nature of the therapeutic option in question, including, the risks posed to patients, and the cost of the therapy.
This superficially may sound fine, but is clearly crafted to lower the bar of scientific evidence for allowing “non-allopathic” treatments into medical practice. The guidelines stress “clinical judgment” rather than evidence-based standards. Further, the only time “sound evidence” is mentioned, it is immediately watered down by qualifying that the type of evidence will depend on the modality in question. Why is that?
The purpose of this language is to allow things like pragmatic studies (unblinded, uncontrolled studies) to serve as evidence for efficacy, something for which they are not designed. This is the sort of thing CAM proponents have been constantly calling for. Andrew Weil has advocated the inclusion of what he calls “uncontrolled clinical observation,” or what has traditional been called “anecdotal evidence.” David Katz from Yale’s Integrative Medicine program has called for “a more fluid concept of evidence.”
The evidence is absolutely clear – the CAM movement is about creating a double standard to allow in medical modalities that are not adequately science based, or to decrease the overall standard of care for medicine with healthcare freedom laws and guidelines that water-down what qualifies as evidence.
Fortunately there has been pushback against these proposed standards. The Canadian Medical Association had this to say:
“The use of complementary and alternative medicine in Canada should be founded on sound scientific evidence as to its safety, efficacy and effectiveness: the same standard by which physicians and all other elements of the health care system should be assessed. When alternative treatment modalities do demonstrate effectiveness, they are usually incorporated into the mainstream of medicine. Therefore, one could argue that complementary and alternative therapies are by definition less demonstrably effective than conventional medical treatment.”
This is exactly correct – CAM modalities by definition have not been adequately shown to be safe and effective, else they wouldn’t be CAM. In other words – we don’t need this special category of treatment. Its only practical functions are marketing and to create a double standard.
Even worse, these standards try to muzzle science-based professionals who would criticize unscientific modalities by including a provision that “non-clinical judgement” should be avoided. This too has caused push-back:
The guidelines may be “interpreted as impressing tight limits on physicians’ ability to state their honest, scientifically sound objections to pseudo-scientific medical theories and ideas,” the Committee for the Advancement of Scientific Skepticism contended. “Their non-conventional medical counterparts feel no such compunction in spreading misinformation about legitimate medical practices such as vaccination, as well as in misrepresenting the scientific standing of dubious non-conventional practices.”
This has also been a long time strategy of the CAM movement – the use of political correctness to silence legitimate criticism. This is a strategy with which I am personally very familiar – attempts at appropriately criticizing unscientific philosophies or claims are often countered with accusations of being closed-minded, bigoted, or even on the take.
Conclusion
The proposed Ontario guidelines are a transparent attempt to water down the science-based standard of modern medicine to allow for what was once called fraud and quackery into medicine, and further to shield such quackery from appropriate science-based criticism. It is no an isolated incident, but is a primary strategy of those hoping to advance CAM into modern medicine.
It is heartening, however, to see that such attempts are now meeting some backlash. Perhaps the CAM proponents have overplayed their hand a bit and those who have been uneasy with the claims of CAM proponents have felt a little more empowered to speak up. Let’s hope this trend continues.
![]()
![]()
![]() <!--<!--
<!--<!--![]()
![]()
![]()
![]()
Scientific American Mind Is Not So Scientific
When Scientific American first announced that they would publish Scientific American Mind, I hurried to subscribe, thinking it would keep me informed about new developments in a field I am passionately interested in. I have enjoyed the magazine, particularly the regular columns, the news items about research findings, the reviews that alert me to books I will want to read, the “Ask the Brains” Q and A, the challenging “Head Games” quiz, and the presentation of many intriguing ideas. The board of advisers is impressive, and the columns by Christof Koch, Scott Lilienfeld, Hal Arkowitz, the Ramachandrans and others have been consistently excellent. Unfortunately, some of the other articles have descended into pop psychology, speculation, poor science and even pseudoscience. Contributing editor Robert Epstein’s articles have particularly raised my blood pressure.
Love-Building Exercises
In December 2009 I was annoyed enough to write this letter to the editor:
After reading Robert Epstein’s article in the last issue, I had to go back to the cover and verify that the word “scientific” was indeed part of the title of your magazine. The Love Building Exercises he recommends are more appropriate to a magazine of fantasy and science fiction.
Two as One — feeling that the two of you have merged?
Soul Gazing — looking into the very core of your beings?
A Mind-Reading Game — wordlessly trying to broadcast a thought to another person?
Love Aura — feeling “eerie kinds of sparks” when your palm is close to another’s?Thought transfer? Auras? Come on! Shame on you for publishing such metaphysical pseudoscientific psychobabble!
They published my letter to the editor with the heading “Hating ‘Love’.” There was no response from the author.
Are You Mentally Healthy?
In a March, 2010, article, “Are You Mentally Healthy?” Epstein presented a screening test that he had developed for mental health disorders and named after himself. He thought his test was more reliable than any of the other tests he found on the Internet because those other tests had not been scientifically validated. His “validation” consisted of his own findings that scores on his test predicted seven important factors related to mental health, such as whether they were employed, how highly they rated their personal and professional success, and whether they had ever been in therapy. (John Nash had been treated for his schizophrenia, but he was employed, won a Nobel prize, and had lasting personal relationships. One wonders how he would have done on Epstein’s test.) Essentially Epstein tried to defend one unvalidated test by showing that it correlates with another unvalidated list of factors.
For fun, I took Epstein’s test. I could see that most of the questions were designed to elicit specific symptoms of depression, mania, anxiety, compulsions, etc. and it appeared to be little more than part of a checklist that a psychiatrist might use to remind him of questions to ask in taking a conventional psychiatric history.
Epstein has not tested people who are known to have mental illness and people who are known to be mentally healthy, but only random people who found his questionnaire on the Internet. He has not defined mental health, much less measured it. He has only shown that his test scores predict a person’s answers to specific questions that are part of the test itself, questions that he personally thinks are related to mental health. People with mental illnesses may not answer the way he thinks that they will. And on the other hand, mentally healthy people might answer the way he thinks only mentally ill people would. The only way to be sure that a survey works is to “test the test”: to see if mentally ill people actually score high on the test. Epstein hasn’t done that.
Any test, questionnaire or instrument must be checked for both reliability and validity: reliability means it will give consistent, reproducible results, and validity means it has been compared to some other standard to ensure that it is actually measuring what it claims to measure. For instance, a new kind of thermometer might reliably give the same result every time, but the readings wouldn’t be valid for diagnosing a fever unless they agreed with the readings on a mercury thermometer. A stopped watch reliably shows the same time each time it is consulted, but it is not valid for telling the time. Epstein may think he has “validated” his questionnaire, but he hasn’t.” He has not shown that the test has any validity for predicting the presence of mental illness.
I tried checking none of the items, and it told me
You haven’t checked off any items, which suggests that your mental health is excellent. If you still have concerns, you can find qualified, licensed counselors and therapists at websites such as Find-a-Therapist.com, GoodTherapy.org, NetworkTherapy.com, PsychologyToday.com, Metanoia.org, AskTheInternetTherapist.com, and TherapistLocator.net. You can also get referrals through your family physician, HMO, or local hospital or clinic. If you are worried that you are losing control of your life, consider taking the test at HowInfantilizedAreYou.com.
Then I tried checking all of the items. This time it told me
In some respects [sic] you scored outside the range of functioning that is usually considered normal. This suggests that you should probably [sic] consult with a qualified mental health professional for further testing or treatment. Area(s) of possible concern (expressed in the diagnostic language that will be familiar to your therapist):
Substance Abuse
Psychosis
Depression
Mania
Bipolar Disorder
Mood Disorder
Phobia
Social Phobia
Obsessive-Compulsive Disorder
Posttraumatic Stress Disorder
Generalized Anxiety Disorder
Anxiety Disorder
Relational Disorder
Sexual Disorder
Eating Disorder
Impulse Disorder
Personality Disorder
Somatoform DisorderYou can find qualified, licensed counselors and therapists at websites such as Find-a-Therapist.com, GoodTherapy.org, NetworkTherapy.com, PsychologyToday.com, Metanoia.org, AskTheInternetTherapist.com, and TherapistLocator.net. You can also get referrals through your family physician, HMO, or local hospital or clinic. If you’re worried that you’re losing control of your life, consider taking the test at HowInfantilizedAreYou.com.
Then I tried checking all the odd-numbered items, resulting in a verdict of pretty healthy but having a possible eating disorder, followed by the same canned universal suggestions.
Checking all the even-numbered items gave me a possible diagnosis of social phobia. Just for the halibut, that time I also reported that I was 10 years old and had a doctorate. That kind of question doesn’t go into the scoring, but Dr. Epstein uses it for his research-by-Internet-stealth. Underlining just how unreliable such research is.
How Do You Handle Stress?
Epstein’s latest article is another example unworthy of Scientific American. In the September/October 2011 issue he gives us “Fight the Frazzled Mind: A new study suggests that preventive, proactive approaches are the most helpful — and that our stress management IQ is painfully low.” The new study is one Epstein did himself and presented at a conference but did not publish in a peer-reviewed journal.
The study looked at 3304 subjects who completed an online test. They were asked to rate, on a 10-point scale, how stressed they were, how generally happy they were, and how much success they had had in both their personal and professional lives. The main body of the test involved questions in four areas of competency: manages sources of stress, practices relaxation techniques, manages thoughts, and prevents stress from occurring. As far as I can see, this identification of four competencies and the corresponding questions are nothing but his own invention. Some examples of individual questions that he thinks can be used to measure those competencies:
- I try to schedule appointments and meetings so that they won’t overlap.
- I schedule some relaxation time every day
- I’m aware that my thinking is sometimes unclear or irrational
- I keep an up-to-date list of things I’m supposed to do.
He says he was surprised by one of his findings: that prevention is by far the most helpful competency when it comes to managing stress. His take-away message is that it is better to avoid stress in the first place than to use techniques like relaxation after stress has developed. I am surprised that he finds this surprising.
He says his study also shows that people who have had training in stress management are better at it, and the greater number of hours of training, the better the skills. He doesn’t explain, elaborate, or quantify. “Stress management training” is not defined.
Then, out of the blue, he offers six strategies he says were “suggested by the new study” to fight stress before it starts:
- Seek [stressors] and kill
- Commit to the positive
- Be your own personal secretary
- Immunize yourself (through exercise, thought management and relaxation techniques)
- Make a little plan (for each day)
- And make a big plan (for the long term)
But these weren’t really suggested by the study, they were strategies that he had already decided ought to be stress-reducing and therefore ought to be included in his questionnaire. Do I smell circular reasoning? And of course, he has no evidence that efforts to adopt these strategies will have any measurable effect.
Then he says the worst news is that on his 100 point scale, people scored an average of 55.3.
If you think of that as a score on an exam at school, that means that on average, people get a grade of F when it comes to managing the inevitable stress they face in their lives.
A Faulty Method
This seems to be Epstein’s modus operandi: he thinks up his own questionnaire to try to measure something, and without even trying to validate it he proceeds to use it in a study, and then gives talks and writes popular articles about his results and gives pop psychology advice allegedly based on the studies. But these studies never get published in peer-reviewed journals and never show up in PubMed. Epstein’s website offers the stress questionnaire and a book of stress relief games, along with tests he has developed to measure such things as “adultness” and “love competency.” No, I’m not making this up! I took the adultness test and found it very entertaining. You might too. His questionnaires are reminiscent of the kind of questionnaires that are ubiquitous in popular magazines, where your score allegedly predicts whether your marriage is likely to last or tells you whether your self-esteem is high or low.
The flaws of this method are obvious, as can be seen in the new “Stress” article. Questionnaires must be validated before they can be used to measure anything. Terms like “stress” must be objectively defined. Self-reports of stress, happiness and success may not correspond reliably to any quantifiable reality. Subjects who self-report as happy, successful and non-stressed can be expected to answer the questionnaire items from the biased perspective of their self-image. And a score on a made-up test can hardly be compared to an F grade in school.
Conclusion
Epstein is much better at self-promotion than at science. In my opinion, Scientific American Mind would be better off without him. Let this stand as an open letter recommending that they remove him from the position of contributing editor and that if they consider publishing any more of his articles, they first submit them to peer review by rigorously scientific psychologists with good critical thinking skills, such as Scott Lilienfeld, who is already on their board of advisers and is also a fellow of the Committee for Skeptical Inquiry and the editor of The Scientific Review of Mental Health Practice. I’m picking on Epstein as a bad example (and a particularly prolific one), but he is not the only offender. Other similarly questionable articles have slipped past the editors. With a little weeding, Scientific American Mind could be what its name promises: scientific.
![]()
![]()
![]() <!--<!--
<!--<!--![]()
![]()
![]()
![]()
Survey says, “Hop on the bandwagon of ‘integrative medicine’!”

A Brief Clinical Vignette
In researching this post, I found an article published nearly two years ago in The Hospitalist entitled Growth Spurt: Complementary and alternative medicine use doubles, which began with this anecdote:
Despite intravenous medication, a young boy in status epilepticus had the pediatric ICU team at the University of Wisconsin School of Medicine and Public Health in Madison stumped. The team called for a consult with the Integrative Medicine Program, which works with licensed acupuncturists and has been affiliated with the department of family medicine since 2001. Acupuncture’s efficacy in this setting has not been validated, but it has been shown to ease chemotherapy-induced nausea and vomiting, as well as radiation-induced xerostomia.
Following several treatments by a licensed acupuncturist and continued conventional care, the boy’s seizures subsided and he was transitioned to the medical floor. Did the acupuncture contribute to bringing the seizures under control? “I can’t say that it was the acupuncture — it was probably a function of all the therapies working together,” says David P. Rakel, MD, assistant professor and director of UW’s Integrative Medicine Program.
The UW case illustrates both current trends and the constant conundrum that surrounds hospital-based complementary medicine: Complementary and alternative medicine’s use is increasing in some U.S. hospitals, yet the existing research evidence for the efficacy of its multiple modalities is decidedly mixed.
My jaw dropped in horror when I read this story. Acupuncture for status epilepticus? There’s no evidence that it works and no scientific plausibility suggesting that it might work. And what does the questionable research suggesting that acupuncture might ease chemotherapy-induced nausea and vomiting or radiation-induced xerostomia (which, if you look more closely at the studies, it almost certainly does not, but that’s a post for another time) have to do with this case, anyway? Nothing. Worse, Dr. Rakel fell for the classic post hoc ergo propter hoc fallacy; i.e., despite his disclaimer, he appears to be implying that, because the child recovered, acupuncture must have contributed to his recovery. He also repeats the classic fallacy that I’ve written about time and time again in the context of cancer therapy, namely that if a patient is using quackery as well as science-based medicine, then either it was the quackery that cured him or the quackery somehow made the conventional medical care work better.
I expect better from an academic medical center like the University of Wisconsin. Unfortunately, increasingly I’m not getting it. Quackademic medicine is infiltrating such medical centers like kudzu.
A survey, a survey, my kingdom for a survey!
One of the most frequently used arguments by promoters of “complementary and alternative medicine” (CAM) or, as it’s more frequently called these days, “integrative medicine” (IM) has nothing to do with science at all. Actually, few of the arguments put forth for “complementing” or “integrating” quackery (which, let’s face it, is all the vast majority of IM really is) with science-based medicine actually have anything to do with science, favoring vague and fuzzy appeals to “holistic” medicine and the “whole patient,” as though it’s not possible to be holistic without adding a heapin’ helpin’ of magical thinking to medicine. It’s the classic false dichotomy: Either we inject a generous dose of woo into our medicine, or medicine remains “non-holistic” or, even worse, reductionistic, and we all know how evil “Western” reductionistic science is, right?

No, one of the favorite tactics used to market CAM/IM comes straight out of the Madison Avenue playbook. Indeed, I can imagine Don Draper of Mad Men cooking it up. It’s a classic argumentum ad populum, whereby CAM/IM advocates try to represent their “product” as being very popular and gaining in popularity every day. These sorts of appeals on the part of CAM/IM frequently emphasize the various subcategories of argumentum ad populum, such as the “bandwagon fallacy,” in which it is argued that, because most people believe something (or because large numbers of people; i.e., a sizable majority) you should believe it too, or at least consider it more seriously. Regular readers should be able to see the problem inherent in that approach. After all, many people believe in ghosts or astrology; the fact that such beliefs are popular does not make them true. The second form of argumentum ad populum is known as “snob appeal,” in which CAM proponents try to persuade you of a conclusion by appealing to what an elite or a select few (but not necessarily an authority) in a society thinks or believes. Of course, I view this variety of argumentum ad populum as more an appeal to authority than anything else, and, as I point out from time to time, an appeal to authority is not always a fallacy, which is why legitimate authorities need to be careful and responsible in what they say. What they say matters to non-experts.
We in medicine have apparently been failing in this respect utterly with respect to CAM/IM.
What led me to this conclusion yet again is a recent survey that’s being flogged in the CAM/IM blogosphere that reports to have found that CAM/IM programs are becoming more common in hospitals and medical centers. My first reaction was almost shruggie-like in that I just wanted to shrug my shoulders and agree with Steve Novella that pseudoscience sells. But then I decided to take a closer look.
What I’m referring to is the 2010 Complementary and Alternative Medicine Survey of Hospitals, a survey that was carried out by the Samueli Institute in collaboration with Health Forum, which is listed as an American Hospital Association Company.” Oddly enough, this survey was not funded by the National Center for Complementary and Alternative Medicine (NCCAM), but rather by the US Army Medical Research and Materiel Command under Award No. W81XWH-10-1-0938. With two wars going on, one would think that the Army would have better things to spend taxpayer dollars on. Apparently you’d be wrong.
For those of you who don’t remember the Samueli Institute, it’s one of the major forces, along with the Bravewell Collaborative, promoting the infiltration of quackademic medicine into academic medical centers. It even describes itself thusly on the cover page of its survey report:
Samueli Institute is a non-profit research organization investigating the safety, effectiveness and integration of healing-oriented practices and environments. We convene and support expert teams to conduct research on natural products; nutrition and lifestyle; mind-body practices; complementary and traditional approaches such as acupuncture, manipulation and yoga; and the placebo (meaning) effect. We support a knowledge network that assists in integrating evidence-based information about healing into mainstream health care and community settings and in creating Optimal Healing Environments.
The “meaning” effect“? Holy Dan Moerman, Batman!
Professor Moerman aside, in a couple of talks I’ve given, I’ve used the Samueli Center for Integrative Medicine at UC-Irvine as an example of just how egregious quackademic medicine can get. Indeed, right there on the SCIM website you can see a homeopath, along with acupuncturists and naturopaths. Some of these might well recommend something called FirstLine Therapy, which is basically a program marketed by Metagenics. Not surprisingly, dietary supplements are part of the program, as is “Ultrameal,” which is billed as “medical food” and takes the form of expensive drink mixes and bars. Yum.
But I digress. What about the survey itself? Let’s go to the Samueli Institute’s press release first:
Hospitals across the nation are responding to patient demand and integrating complementary and alternative medicine (CAM) services with the conventional services they normally provide, according to the results of a new survey released today by Health Forum, a subsidiary of the American Hospital Association (AHA) and Samueli Institute, a non-profit research organization that investigates healing oriented practices. The survey shows that more than 42 percent of responding hospitals indicated they offer one or more CAM therapies, up from 37 percent in 2007.
Note how this is a clever combination of the bandwagon appeal and an appeal to authority. After all, there is “patient demand,” and the authorities (i.e., hospitals) are responding. The unspoken subtext is the assumption that hospitals wouldn’t respond to such a demand if there weren’t something to it. They are, after all, health care institutions made up of health care professionals, right? Well, yes, but hospitals are also businesses, and many of these health care professionals have either bought into the myth that “holism” and improving the doctor-patient relationship requires woo, or they are shruggies.
Meanwhile, CAM/IM apologists and supporters are jumping all over this survey as “evidence” that they are winning. John Weeks of the Integrator Blog, for instance, crows:
The most significant data point here is that 74% say that “clinical effectiveness” is a top reason for inclusion. This growth took place in a down economy and despite the lack of good payment models for CAM. These findings will be interesting to view after new incentive structures that might support CAM inclusion kick in with the growth of accountable care organizations (ACOs).
“Clinical effectiveness”? Based on what? Certainly not science in most cases.
In any case, the story has gotten some traction in the mainstream media, such as the L.A. Times, which, tellingly, chose to report on the survey on its Money & Company blog under the title Alternative medical services growing at U.S. hospitals, quoting widely from the joint press release of the AHA and Samueli Institute.
But does the survey actually show what it claims? Let’s go to the report itself. The first thing I noticed when I read the report was that it’s full of the typical “bait and switch” language of CAM designed to inflate the numbers of people who apparently use “CAM modalities.” For instance, diet, exercise, and the like are represented deceptively as being somehow “alternative” when their utility not only can be studied by science but has been studied by science. None of this is surprising, but it is harmful in that it applies a layer of “mystery” and “danger” to modalities that physicians have been prescribing their patients for a long time, such as better nutrition and more exercise. These modalities are, in effect, “woo-ified.” Then, they are lumped together with the real woo, such as acupuncture, homeopathy, and “energy healing,” in order to provide legitimacy by association. For instance, if you look at Figure 2, you’ll see that natural products are the most commonly reported CAM modality, which tells me that the supplement industry’s marketing hype has been effective. More tellingly, other than chiropractic, all of the top nine modalities are nothing that couldn’t be considered SBM. True, homeopathy just barely squeaks into the top ten at number ten, but only 1.8% of adults in the U.S. have reported using it. (I suspect the number would be higher in Europe.) Where’s traditional Chinese medicine? Where’s acupuncture? Where’s “energy healing”? Apparently none of them made the top ten. For instance, if you go to the 2007 National Health Interview Survey Report, you’ll find that only 1.4% reported using acupuncture; 0.4% reported using naturopathy; 0.1% reported using Ayurveda; and 0.5% reported using reiki.
No wonder the bait and switch move is necessary, at least if CAM practitioners want to represent the popularity of their methods as being higher than single digit percents (or in some cases higher than 1%).
Here’s how the survey was done:
The 2010 Complementary and Alternative Medicine Survey of Hospitals, a 42-question instrument, was mailed to 5,858 hospitals from American Hospital Association’s inventory of opened and operating member and nonmember hospitals in March 2010. Respondents had the option to either complete the survey online or mail back a hard copy. A total of 714 responses were received for a response rate of 12%. Of responding hospitals, 299 (42%) stated that they offered one or more CAM therapies in the hospital—which could be either in the form of services provided to patients or employees.
Does anyone see the problem here? It’s fairly obvious, namely the response rate. It’s pretty hard to say much of anything based on a 12% response rate. Basically, all we can say is that 42% of the respondents have a CAM program of some sort or another, but we have no idea whether the respondents are a representative sample. Indeed, they almost certainly are not; there is probably major selection bias going on here, with respondents more likely to be the ones who have some sort of CAM program. Just the geographic distribution of responses makes me wonder, though, with 23% coming from the Midwest and only 11% coming from West Coast states. Later in the report, it is pointed out that “most of the hospitals responding to this survey would be considered ‘early adopters’” who are, apparently, adopting CAM “because they believe it’s the right thing to do or because it’s important to respond to the needs of their communities and patients.” Clearly, this is not a representative sample. Be that as it may, it can still be informative to examine this non-representative sample. For example, the “bait and switch” continues here, with the top six outpatient modalities being:
- Massage therapy
- Acupuncture
- Guided imagery
- Meditation
- Relaxation
- Biofeedback
And the top six inpatient modalities being:
- Pet therapy
- Massage Therapy
- Music/art therapy
- Guided imagery
- Relaxation training
- Reiki and therapeutic touch
The authors of the survey report conclude with amusing understatement:
Looking at the top modalities offered in hospitals it is clear that hospitals are “playing it safe” and starting with fairly conservative and non-invasive therapies to appeal to the broadest range of patients and consumers in the their community. Pet therapy has been growing in popularity. Massage therapy is provided predominantly for pain and stress management and for cancer patients, according to the American Massage Therapy Association’s 2007 Survey of Massage Therapy Utilization in Hospitals.
Other key findings include:
- Majority of respondents offer wellness services for patients and staff, including nutritional counseling, smoking cessation, fitness training and pastoral care;
- Massage therapy is in the top two services provided in both outpatient and inpatient settings;
- The majority of hospitals that offered CAM were urban hospitals (72 percent); and
- Seventy-five percent cited budgetary constraints as the biggest obstacle for implementation of CAM programs.
It is rather instructive, though, to look at the differences between inpatient and outpatient. First of all, who decided that “pet therapy” was in any way alternative? It’s not really “therapy,” either: it’s a great way to raise spirits among hospitalized patients, but lumping it in as a “CAM” therapy seems a major stretch to me. (If pet therapy is an “alternative” or “integrative” therapy, then sending hospitalized patients a card and flowers to lift their spirits must also be alternative or integrative therapy.) Secondly, it is interesting how reiki and therapeutic touch are major offerings in the inpatient realm but not in the outpatient realm. Very likely this is due to the decades-long infiltration of therapeutic touch in the nursing profession, leading too many nurses to come to believe that they can somehow realign a patient’s energy field to healing effect by waving their hands around. Reiki fits right into that, particularly given that reiki practitioners have been making a concerted effort to get into hospitals and offer their “services” to patients.
Money vs. ideology
It’s even more instructive to look at the reasons given for starting up a CAM program. Inevitably, financial considerations, plus popularity and a perceived demand among patients, are among the handful of factors that predominate:
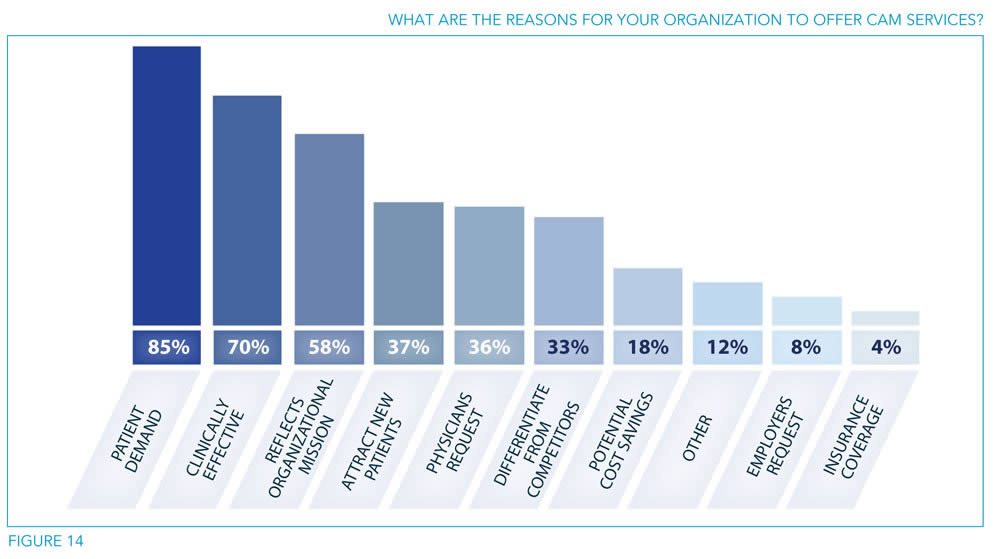
Look at what comes in as number one: patient demand at 85%. None of this is surprising, given that in the introduction it is stated:
The American public is also demanding that their hospitals offer more than conventional allopathic health care and begin to integrate CAM therapies into the care they receive in the hospital. In response, hospitals have been looking to meet the needs of their communities. The demand for CAM services is significant, even though insurers may not cover all services or products, with the American public spending approximately $12–19 billion on CAM providers and a total of $36–47 billion on all services and products combined.
Which at first suggested to me that it’s almost all about the business. There’s a lot of money to be made in CAM, and it’s paid for out of pocket. It’s also instructive to look at the reasons given for choosing the CAM modalities offered:

There are, however, a couple of anomalies here. Most prominent, given that only 27% state that market research drove their decision to offer CAM, one wonders how all the others who didn’t do any market research (78%) knew that there was enough patient demand to justify spending the money to offer specific CAM services. In any case, I consider it also telling that the survey reports that 85% will use patient satisfaction as a metric to evaluate the CAM program while only 42% plan on evaluating health outcomes and 31% will evaluate quality. Don’t get me wrong, patient satisfaction is important, and we measure it for science-based medicine. However, there’s something wrong when twice as many hospitals with CAM programs will be looking at patient satisfaction as will be looking at health outcomes.
Perhaps the most interesting part of this study suggests that it may actually not be all about the money, despite the listing of how lucrative CAM can be. For example, only 57% of facilities will be using volume as a criterion for evaluating their CAM program. Is there a clinical program on earth (or at least in the U.S.) that doesn’t use volume as part of its criteria for evaluating it? It may be one of many, and it might not even be one of the more important criteria, but it’s usually a significant criterion. Adding to this, only 39% will use revenue; 20% will use profit; and 8% will use market share. To me these suggest that perhaps CAM is indeed more ideological than financial, particularly when coupled with the finding that 75% of hospitals reported that budgetary constraints are the biggest obstacle to implementing a CAM program, even though such programs can cost as little as $200,000 to start up. (One notes, in contrast, that only 43% reported that a “lack of evidence-based studies” was a major obstacle.) No wonder quackademic medicine is trying so hard to entice third party payers to reimburse for their services; if that were to happen, no doubt many CAM programs that are currently not financially viable will become viable. Perhaps, for as unrepresentative a sample as was surveyed, this survey serves the inadvertent purpose in providing evidence to suggest that the infiltration of quackademic medicine is not driven primarily by money, as skeptics and supporters of SBM (myself included) have on occasion speculated.
Maybe it really is about the ideology.
![]()
![]()
![]() <!--<!--
<!--<!--![]()
![]()
![]()
![]()