
Sam had wanted to see the painted houses of Burano since the first day he read about them on the Internet. We decided a day off the main island would do us well and so after a charming little breakfast at our BB we headed out. We took the Vaparetto1 to the Fond Nova stop then got on the Vaparetto to Burano. The ride was long and hot but there was so much to look at it didnrsquot matter.Fin
Day 29 July 13 Venice
We started the morning walking along the Venice Boardwalk seeing some cruise ships come in others docked. We tried to have an early morning to see St. Marks somewhat empty and to see the actual church which had been too crowded the last time we were there. Alas everyone including the day cruisers had the same idea. Although we arrived just after nine the line up stretched all the way acros
Day 30 July 14 our last day
We headed straight over to Murano the next day to see the legendary glass. Sam refused to follow the crowds stepping off the boat to a glass museum where we were all being directed by an enthusiastic promoter even though I was afraid we would not get to see a glass blowing demonstration Instead we began wandering the island looking at all of the glass dodads enjoying the atmosphere.Almost i
Days 31 32 July 15 16 The Journey Home
There was really only time to pack have breakfast and start the long journey home in the morning. We packed carefully my journals and our wine glasses in our carryons. We walked over to the nearest vaparetto stop where we could catch a vaparetto to the airport. These take separate tickets which I wasnrsquot aware of but it wasnrsquot a big deal still a cost effective way to travel. The
A Disastrous Start I’m Not Sure I’m Going to Like Interrailing
As I hadn't quite paid off the debts that I had clocked up going round the world oh for the State Bank Victoria this trip was going to be courtesy of my flexible friend. That and the fact that it was going to be some time before I got my first paypacket meant that I was going to be travelling on a serious budget. Apparently it's a crime for interrailers to have money so I thought it should
Day 22 July 5 Volestra and the best dinner of our lives
I woke up and informed Sam I was not up for a hike into the foothills. He wanted to go anyway. We made loose plans to meet in Volastra I was going to bus up and this would be the midway point in his hike.I mistimed the trains and busses and ended up arriving in Volastra at about 230. Turns out Sam arrived at 145 waited until 215 we had agreed he would wait until 2pm and then hiked dow
Day 24 July 6 Lucca
We got a later start than expected. We ate breakfast on the terrace finishing all of our supplies and rested for a bit then picked up final paninis at Il Forno for our lunch. All this leisure resulted in missing the last train I had carefully planned our potential routes around. though I had carefully planned the shortest route to Lucca all of the plans fell apart and we ended up waiting half
Day 24 July 7 San Giminano and a luxurious suprise
We awoke the next morning and enjoyed a fabulous breakfast at the BB egg cheese meats buns fruit all delivered in the breakfast room by a charming Italian ldquomammardquo who you could tell just loved her life and loved serving breakfast to her guests. We planned to spend the morning in Lucca so we started walking around some more.. We played a game trying to find a street without a s
Hispanic Males Entering Medical School Record Numbers – Terra.com
 Terra.com | Hispanic Males Entering Medical School Record Numbers Terra.com According to the to data released by the Association of American Medical Colleges Hispanic males have become the top minority to enroll into medical schools ... Hispanics Enter Med School in Record NumbersMedPage Today Medical School Enrollment Shows Diversity GainsNewswise (press release) Medical Schools Slowly GrowInside Higher Ed |
Latino Men See Dramatic Jump as First-year Medical School Students – Diverse: Issues in Higher Educatio
Diverse: Issues in Higher Educatio | Latino Men See Dramatic Jump as First-year Medical School Students Diverse: Issues in Higher Educatio While entering medical school is a significant accomplishment for anyone, it was a monumental feat for Godoy, whose childhood was split between schoolwork ... |
Duke’s medical school expands; new Learning Center to centralize facilities … – My Fox 8
Duke's medical school expands; new Learning Center to centralize facilities ... My Fox 8 ... exam rooms to surgery suites to emergency rooms. The new building also will centralize medical school facilities that have been spread across campus. |
Quinnipiac sets an ambitious goal for its future medical school – The Connecticut Mirror
 Milwaukee Business Journal (blog) | Quinnipiac sets an ambitious goal for its future medical school The Connecticut Mirror NORTH HAVEN--As if creating a medical school from scratch in just four years isn't ambitious enough, Quinnipiac University has ... OUR VIEW: Planning for enough physicians for futureBristol Press 50 Integrated Delivery Systems to KnowBecker's Hospital Review Our view: University making needed effortNorwich Bulletin |
Uff Da! The Mayo Clinic Shills for Snake Oil
A couple of weeks ago, in a review of the Mayo Clinic Book of Home Remedies, Harriet Hall expressed relief that she hadn’t found any “questionable recommendations for complementary & alternative medicine (CAM) treatments” in that book:
Since “quackademic” medicine is infiltrating our best institutions and organizations, I wasn’t sure I could trust even the prestigious Mayo Clinic.
The Home Remedies book may be free of woo, but Dr. Hall was right to wonder if she could trust the Mayo Clinic. About a year ago I was asked to comment on an article in the American Journal of Hematology, in which investigators from the Mayo Clinic reported that among a cohort of lymphoma patients who were “CAM” users,
There was a general lack of knowledge about forms of CAM, and about potential risks associated with specific types of CAM…
This suggests the need to improve access to evidence-based information regarding CAM to all patients with lymphoma.
No surprise, that, but I couldn’t help calling attention to the paradox of one hand of the Mayo Clinic having issued that report even as the other was contributing to such ignorance:
The Mayo Clinic Book of Alternative Medicine details dozens of natural therapies that have worked safely for many patients in treating 20 top health issues. You may be surprised that Mayo Clinic now urges you and your doctor to consider yoga, garlic, acupuncture, dietary supplements and other natural therapies. Yet the record is clear. Many of these alternative therapies can help you achieve reduced arthritis pain, healthier coronary arteries, improved diabetes management, better memory function and more.

Nor could such a paradox be explained by the right hand not having known what the left was doing: Brent Bauer, MD, the Director of the Mayo Clinic Complementary and Integrative Medicine Program, is both the medical editor of the Book of Alternative Medicine (MCBAM) and a co-author of the article in the AJH.
As chance would have it, I had picked up a copy of the latest (2011) edition of the MCBAM only a couple of days before Dr. Hall’s post. Does it live up to its promises? Do its “straight answers from the world’s leading medical experts” respond to “the need to improve access to evidence-based information regarding CAM?” Let’s find out. In some cases I’ll state the implied questions and provide the straight answers.
The Introduction
In the Introduction, Dr. Bauer asserts that “an opportunity has risen that may hold the promise of a new paradigm for better health.” He makes several, implicit or explicit assertions that are repeated throughout the book:
The best way to manage an illness is to prevent it from happening in the first place…It’s in this environment—one in which Americans are seeking greater control of their health—that we’ve seen explosive growth in the field of alternative medicine. People are looking for more “natural” or “holistic” ways to maintain good health…
The implied question: Should people be looking for such things? Is there anything useful in “alternative” (or “natural” or “holistic” or “integrative”) medicine, different from what modern medicine and public health have learned by rational inquiry, for preventing an illness?
The straight answer: No.
Dr. Bauer goes on:
By combining the best of complementary and conventional health care practices to meet your individual needs, you’ll be practicing integrative medicine.
The implied question: Do the world’s leading medical experts know which are the “best complementary” practices, or even if any of them work?
The straight answer: No. Most “alternative” or “complementary” practices are known not to work or are vanishingly unlikely to work. Exceptions are a few botanical medicines, but these are overhyped and are disadvantageous compared to purified, precisely dosed, well-studied pharmaceuticals. Other claimed exceptions, such as rational diets, exercise, manual techniques for musculoskeletal complaints, and relaxation techniques, are not “alternative” at all.
Dr. Bauer again:
…an increasing number of treatments once considered “on the fringe” are slowly being incorporated into conventional medicine.
The implied question: If this true, is it because those treatments have been shown to be effective?
The straight answer: No. Over the past several years, an increasing number of treatments once considered promising by naïve “alternative medicine” proponents have been tested in clinical trials and shown to be ineffective. R. Barker Bausell, the former Director of Research at the University of Maryland Complementary Medicine Program, reviewed this literature for his 2007 book, Snake Oil Science; the Truth About Complementary and Alternative Medicine:
Because of its emphasis upon high-quality scientific evidence, this book could not have been written in April 1999…Now, however, enough evidence has accumulated to permit the first scientific evaluation of complementary and alternative medicine. [p. xv]
And what did Bausell’s evaluation reveal?
There is no compelling, credible scientific evidence to suggest that any CAM therapy benefits any medical condition or reduces any symptom (pain or otherwise) better than a placebo. [p. 254]
Edzard Ernst, the most prolific “CAM” researcher of the past 20 years, offered similar conclusions in his 2008 book, co-authored with Simon Singh, Trick or Treatment: the Undeniable Facts about Alternative Medicine:
The bottom line is that none of the above treatments (herbal medicine, chiropractic, acupuncture, homeopathy) is backed by the kind of evidence that would be considered impressive by the current standards of medical research. Those benefits that might exist are simply too small, too inconsistent and too contentious. Moreover, none of these alternative treatments (apart from a few herbal medicines) compare well against the conventional options for the same conditions. This dismal pattern is repeated [for] many more alternative therapies. [pp. 238-9]
Back to the Mayo Clinic’s Bauer:
…what’s considered alternative today may be conventional tomorrow. In addition, using a particular therapy to treat one condition may be an accepted medical practice, but using it to treat another condition may not. A case in point is chiropractic care. There are numerous studies to back up the effectiveness of chiropractic therapy for low back pain. However, use of chiropractic techniques to treat high blood pressure would still be considered an alternative practice by many because there’s not sufficient evidence that it’s effective.
The implied question: Does this mean that there is likely to be sufficient evidence in the future? In other words, is there any anatomic or physiologic basis for predicting that chiropractic “care” might treat high blood pressure?
The straight answer: No. The idea is so implausible (and dangerous, in the case of neck manipulation) that it would be unethical to perform trials.
In the introduction, Bauer also makes these promises:
The purpose of Mayo Clinic Guide to Alternative Medicine 2011 isn’t only to inform you about various products and practices, but to guide you as to which appear to be of benefit and may help treat or prevent disease and which are of no benefit and could even be dangerous.
Let’s see whether those promises are fulfilled as we move on to a few specific treatments.
“Our Top 10″
Sorry that the picture below didn’t come out sharply enough, but here are the two paragraphs at its top—a weasel wordfest similar to the book as a whole:
Here’s a brief rundown of what we consider to be the best integrative therapies at this point in time.
Research into complementary and alternative medicine is rapidly evolving. New studies are coming forward on an increasingly frequent basis and, many times, new studies conflict with older studies. To complicate matters even more, different forms can have different effects. This makes it difficult to state with authority which therapies are truly “the best.” However, we’ve listed what we consider to be the top 10.

Notice that the list is in alphabetical order, so we’re not told which of these ‘therapies’ the Mayo Clinic really likes. Notice, also, that the column on the right has to do with popularity, not validity. Most of the Top 10 are not “CAM” at all, as long as they’re used for rational purposes: guided imagery, hypnosis, meditiation, music therapy, spirituality and yoga for “stress” or pain, spinal manipulation for low back pain, massage for pain, and Tai chi for “balance and strength.”
On the other hand, aren’t most people expecting more for their “CAM” dollars? Can’t guided imagery, for example, recruit lymphocytes to fight cancer? Doesn’t massage remove toxins and “increase cytotoxic capacity“? Can’t intercessary prayer improve outcomes of serious diseases? Isn’t spinal manipulation also for health maintenance and for treating ADHD, asthma, infantile colic, otitis media, and many other problems? The Mayo Clinic Book of Alternative Medicine offers no straight answers—if it offers answers at all—to such questions.
The book has a system of “stop-lights” to let readers know whether it considers various methods to be “generally safe for most people to use, and studies show it to be effective” (green), “use the therapy with caution” (yellow), or “not to use the treatment or to use it very carefully and only under a doctor’s supervision” (red). The last recommendation is repeated throughout the book:
Even when a green light is present, it’s still important that you discuss the treatment with your doctor and use it appropriately.
Hmmm. Readers are also told in this book that “a naturopathic physician is a primary health care provider trained in a broad scope of naturopathic practices in addition to a standard medical curriculum” (the straight answer: No), and will have been assured elsewhere that “The proper title for a doctor of chiropractic is ‘doctor’ as they are considered physicians under Medicare and in the overwhelming majority of states.”
Let’s briefly look at the book’s discussions of a few methods.
Acupuncture
The book gives this Top Tenner a “shining green light”:
Our Take
Acupuncture has been used at the Mayo Clinic since the 1970s. Mayo Clinic has licensed acupuncturists on staff. When performed properly by trained practitioners using sterile needles, acupuncture has proved to be a safe and effective therapy. A review of acupuncture by the World Health Organization found it was an effective treatment for 28 conditions and there was evidence to suggest it may be effective for several more.
The straight answer: No.
Chiropractic
The “Hands-on Therapies” chapter was written by Ralph Gay, MD, DC. Here is his entire description of the conceptual basis of chiropractic:
Chiropractic treatment is based on the concept that restricted movement in the spine may lead to pain and reduced function. Spinal adjustment (manipulation) is one form of therapy chiropractors use to treat restricted spinal mobility. The goal is to restore spinal movement and, as a result, improve function and decrease back pain.
Dr. Gay has somehow omitted any discussion of the central dogma of chiropractic: the subluxation. He is aware of it, of course; elsewhere he calls it “a good theory.”
Here, Dr. Gay comments on reflexology:
Among most conventional doctors, the theory behind reflexology is a little difficult to grasp.
Uh, no kidding, but that doesn’t stop him from asserting that “preliminary evidence” for reflexology reducing menopause symptoms requires “further research.” What the hay, asks Dr. Gay, “Why does any form of treatment work?”
Energy Therapies
Nurse Susanne Cutshall informs us that
Energy based therapies may be among the most controversial practices because of the difficulty in convincingly using any biophysical means to measure the effects of some therapies. However, active investigations are being conducted at academic medical centers, including Mayo Clinic, and energy medicine, in general, is gradually gaining popularity.
Ah, the magical effects of the euphemism (”difficulty”), the pseudoscientifc (”biophysical means”), the weasel words (”convincingly,” “some”), and the bait-and-switch (”active investigations” begets ”popularity”). You won’t learn, in this discussion, of the diffculty in convincingly using any human means to measure the effects of some therapies.
Homeopathy
Rheumatologist Nisha Manek discusses “other approaches”: Ayurveda, homeopathy, naturopathy, and Traditional Chinese Medicine:
Treatments that comprise alternative medical systems focus on prevention and on achieving a healthy ‘balance.’ They promote diet, exercise, sleep, and daily routines to maintain wellness and encourage healing.
Jeez, there musta been something other than their alternative medical systems to explain why China and India have suffered from terrible plagues and other ills, even within the last few decades. Not to put too fine a point on it.
What about those medical systems that we honkies can call our own? We’ve already heard from the Mayo regarding naturopaths. Homeopathy gets a “yellow light” (how responsibly cautious!):
Homeopathic medicine is popular. However, it lacks good studies to prove its effectiveness. Studies that have been done have generally been small and have produced conflicting results. In general, the scientific community also finds the theories on which homeopathic medicine is based questionable and difficult to accept. These factors have kept it from being widely accepted into mainstream medicine.
Phew. Such language—with its suggestion that it is the lack of good studies that holds homeopathy down, its implicit call for more studies, its coy suggestion that it isn’t so much that the “theories are questionable” but that the scientific community is, well, too closed-minded to accept them—is so prevalent in this book that it makes me weary, so let’s quickly wrap this up. The straight answer: No.
The Need to Obfuscate
I should mention that not every method discussed in this book is given a green or even a yellow light. I can imagine that proponents are accusing me of selective quoting, and that’s true to an extent. It is a justifiable extent, however, because what I’ve discussed is more than sufficient to disqualify the Mayo Clinic authors from any claim to responsible reporting.
What’s most noticeable about the tone of the book is it’s ponderous, ditzy blandness (if there is any hope that woo-philic readers will tire when they finally realize that they are being treated like small children, this book will be invaluable). Such blandness, of course, is common to apologetic, quackademic expositions. So are the misleading language devices mentioned above (and more: chiropractic becomes “chiropractic care”; homeopathy becomes “homeopathic medicine,” which “seeks to stimulate the body’s ability to heal itself by giving small doses of highly diluted substances [that] are derived from natural substances,” and so forth).
“Today’s New Medicine,” as the Mayo book also calls it, is thus new because, well, it’s promoters call it “new“. No surprise that the authors tout the Bravewell Collaborative’s Consortium of Academic Health Centers for Integrative Medicine, a great wellspring of Quackademic Newspeak. But we’ve known that the Mayo Clinic has been in bed with Bravewell for years.
![]()
The Cargo Cult of Acupuncture
Bloodletting, of course, was a major aim of early vessel therapy and is frequently described in the Su wen.1
Paul U Unschuld
“Cargo cult” is a metaphor that describes the act of imitating an activity or a practice without any insight into the underlying principles. In the literal sense, it refers to a magico-religious practice observed in tribal societies, where the members ritually imitate the activities of a technologically-advanced society they had contact with, so that they can magically draw their material wealth. For instance, after WWII, indigenous tribes in New Guinea who had come in close contact with cargo planes, started to build landing strips and populated them with plane-like effigies that were made of straw, bamboo, and coconuts, so that they can magically lure the passing planes.2 The term “cargo cult science” was introduced by Richard Feynman in a speech at Caltech in 1974 to describe pseudoscientific studies in which all the superficial aspects of a scientific inquiry are adhered to, but the underlying principles are not scientific. He classified many educational and psychological studies as such, for having the appearance of academic research but lacking the principles of a scientific inquiry.3
Another example of cargo cult science is the plethora of two-arm acupuncture studies that compare a needling regimen using the traditional concepts, and compare it with a non-interventional placebo. These studies might have the appearance of clinical research, but they are inherently flawed and inconclusive, because they do not rule out the possibility that the observed results are mainly due to the painful stimulus and injury caused by a needle, which can occur regardless of the insertion point. Indeed, an acute noxious stimulus from a prickle, heat, or any other painful stimulus – almost anywhere on the skin – can attenuate the perception of pain in another area of the body through a reflex called “counter-irritation,” also called the “pain-inhibiting-pain effect” or “diffuse noxious inhibitory control” (DNIC).4 DNIC was extensively studied by Fauve et al. in the 1980s, who showed in mice that it has an effect equivalent or superior to that of glucocorticoids.5,6
Counter-irritation has been known since antiquity, and is at the base of many noxious folk remedies, such as the application of cautery, blistering and moxibustion (the burning of dried Artemisia annua on the skin) to name but a few, whereby “one pain masks another.”7 These modalities were once widely used, generally in an attempt to reduce inflammation.9 It is therefore plausible that the nonspecific effects observed in some types of acupuncture are also linked to DNIC, since some authors have reported that acupuncture is only effective in producing analgesia when the stimulation itself is of a sufficient intensity to cause an unpleasant sensation. The DNIC induced by needles is believed to be mediated by the release of endogenous opioid neuropeptides and/or monoaminergic neurotransmitters, mainly because naloxone, a central and peripheral opioid receptor antagonist, is reported to reverse its effects.10,11 A true interpretation of this finding invalidates the traditional lore of the meridian-and-points system, and indicates that any needling regimen can lead to outcomes associated with DNIC. This finding echoes the position of Felix Mann, MD, the founder of the British Medical Acupuncture Society, who after decades of practice reached the conclusion that putting needles in “wrong” places was as effective as a “correct” treatment. He therefore wrote that “traditional acupuncture points are no more real than the black spots a drunkard sees in front of his eyes.”12
There is also credible evidence that the stimulation of a myofascial trigger point (TrP), meaning a localized, hyperirritable nodule nested within a palpable taut band of skeletal muscle or fascia,13 can evoke short-term anti-nociceptive effects on the same segmental dermatome.14 This local hypoalgesic effect is reported to be greater than stimulation at remote dermatomes.15 It is based on this finding, that Janet Travell, MD, (1901-1997) began needling hyperirritable points with syringes in in the 1940s, injecting them first with procaine.16 Procaine was later replaced by saline solution,17 which was later replaced by “dry needling” (TrP-DN ) — without any fluid in the syringe.18,19 Although the dermatomal distributiosn of anti-nociceptive effects do not correspond to the distribution of the Chinese meridians, they do affect the outcome of two-arm studies because any needling regimen in the same dermatome should lead to similar results. Therefore, two-arm studies cannot rule out the possibility that the observed results are due to anti-nociceptive effects on the same segmental dermatome, which can occur regardless of the classical theories for point selection and means of stimulation.20
In addition, both laboratory and clinical evidence have recently shown the existence of two-way interactions between the nervous system and the innate immunity. There is experimental evidence showing that percutaneous and transcutaneous neurostimulation can inhibit macrophage activation and the production of pro-inflammatory cytokines.21 Kevin J Tracey, MD and his collogues at Feinstein Institute for Medical Research have shown that an increase in the production of Acetylcholine (ACh) can inhibit the synthesis of TNF and other pro-inflammatory cytokines in organs rich in cells of the monocyte-macrophage system.22 Tracey argues that Ach interacts with members of the nicotinic ACh receptor (nAchr) family, in particular with the alpha-7 subunit (?7nAchr), which is expressed not only by neurons, but also macrophages and other cells involved in the inflammatory response.23 It is therefore conceivable that the anti-inflammatory actions that have been associated with needling – and have been used to justify the traditional concepts of acupuncture – are directly or indirectly mediated by neurostimulation and inflammatory macrophage deactivation, and can occur with transcutaneous or percutaneous neuromodulation anywhere proximal to nerves.24 This is consistent with the hypothesis of George A. Ulett and Songping Han, who argued that certain effects of needling, especially in the ear, might be explained by a “broad parasympathetic effects” due to the stimulation of vagus nerve, which also innervates the ear.25 Again, two-arm studies cannot rule out the possibility that the observed results are due to the broad neurostimulatory effects of needling, and regardless of the needling regimen.
In sum, for the reasons stated above, two-arm acupuncture studies that compare a traditional regimen with a non-interventional placebo are inherently inconclusive. I would further argue that the regimen used in these studies is not even reflective of the traditional methods, because the loci of cautery, blistering, cupping, moxibustion and acupuncture might have been selected simply because they were particularly sensitive and painful, and the alleged analgesic and anti-inflammatory effects of traditional regimens are not achievable by the “soft needling” technique used in clinical studies today. These studies unequivocally use quasi-unperceivable, painless, filiform, silicon-coated needles for ethical reasons and to prevent dropouts. This type of “acupuncture without tears” amounts to what Arthur Taub has suitably called “nonsense with needles.”26
Finally, the most compelling argument to qualify acupuncture of a cargo cult, is the fact that its apostles remain obstinately faithful that someday, someone will prove that “astrology with needles” is a panacea that can naturally restore health and longevity. This is despite the fact that well-conducted three-arm clinical trials that used sham controls with needle insertion at “wrong” points (points not indicated for the condition) or non-points (locations that are not known acupuncture points) along with a non-interventional control group, have failed to demonstrate that there is a reliable difference between sham and “true” needling. Three well-designed three-armed randomized controlled clinical trials with 302, 270, and 1007 patients, respectively, have demonstrated that acupuncture and sham acupuncture treatments were more effective than no treatment at all, but there was no statistically significant difference between true and sham acupuncture,27,28,29 suggesting that it does not have unique effects on the central nervous system, or on pain and pain modulation.30 These studies indicate that the “meridional theory” is of low importance, and does not lead to specific therapeutic effects.31,32 The most recent challenge came from a review article in the New England Journal of Medicine which concluded that acupuncture’s specific therapeutic effects – if any – are small, and its benefits are mostly attributable to “contextual and psychosocial factors, such as patients’ beliefs and expectations, attention from the acupuncturist, and highly focused, spatially directed attention on the part of the patient.”33
I see the pointless studies that aim to validate notions that date of Galen’s era, and hear the irrational narrative of the apostles of this cargo cult at the twilight of a dying hope, and I think of Baudelaire’s morose elegy to “The Swan:”
A swan which from its cage had made escape
Patting the torrid blocks with webby feet,
Trailing great plumes of snow, while beak agape
Tumbled for water in the parching street;Wildly it plunged its wings in dust again,
Mourning its native lake, and seemed to shrill:
“Lightning, when comest thou? and when, the rain?”
Strange symbol! wretched bird, I see it still.34
Charles Baudelaire (1821 – 1867), Flowers of Evil
1. Unschuld PU. Huang Di Nei Jing Su Wen: Nature, Knowledge, Imagery in an Ancient Chinese Medical Text. University of California Press. 2003
2. Lawrence P. Road belong cargo: a study of the Cargo Movement in the Southern Madang District, New Guinea. Manchester University Press, 1964.
3. Feynman RP. Surely You’re Joking, Mr. Feynman! (Adventures of a Curious Character). W. W. Norton & Company. 1997.
4. Follett K. Neurosurgical Pain Management. Elsevier Health Sciences. 2004
5. Fauve RM, Fontan E, Hevin MB, Saklani H, Parker F. Remote effects of inflammation on non-specific immunity. Immunol Lett. 1987;16(3-4):199-203.
6. Fauve RM. Endogenous counterinflammation and immunostimulation [in French]. Pathol Biol (Paris). 1987;35(2):190-194.
7. Wand-Tetley JI. Historical methods of counter-irritation. Ann Phys Med 1956;3:90–8
8. Le Bars D, Dickenson AH, Besson J-M, Villaueva L. Aspects of sensory processing through convergent neurons. In: Yaksh TL, ed. Spinal afferent processing. New York: Plenum, 1986: 467–504.
9. Holden AV, Winlow W. The Neurobiology of Pain: Symposium of the Northern Neurobiology Group, Held at Leeds on 18 April 1983. Manchester University Press. 1984.
10. Pomeranz B, Chiu D. Naloxone blockade of acupuncture analgesia: endorphin implicated. Life Sci. 1976;19:1757-1762.
11. Zhou ZF, Du MY, Wu WY, Jiang Y, Han JS. Effect of intracerebral microinjection of naloxone on acupuncture- and morphineanalgesia in the rabbit. Sci Sin. 1981;24:1166-1178.
12. Mann F. Reinventing Acupuncture: A New Concept of Ancient Medicine. Butterworth-Heinemann; 2 edition. 2000.
13. Simons DG. Review of enigmatic MTrPs as a common cause of enigmatic musculoskeletal pain and dysfunction. J Electromyogr Kinesiol 2004; 14: 95–107.
14. Srbely JZ, Dickey JP, Lee D, Lowerison M. Dry needle stimulation of myofascial trigger points evokes segmental anti-nociceptive effects. J Rehabil Med. 2010 May;42(5):463-8.
15. White PF, Craig WF, Vakharia AS, Ghoname E, Ahmed HE, Hamza MA. Percutaneous neuromodulation therapy: does the location of electrical stimulation effect the acute analgesic response? Anesth Analg. 2000 Oct;91(4):949-54.
16. Travell J, Rinzler S, Herman M. Pain and disability of the shoulder and arm: treatment by intramuscular infiltration with procaine hydrochloride. JAMA. 1942;120:417-422.
17. Sola AE, Kuitert JH. Myofascial trigger point pain in the neck and shoulder girdle. Northwest Med. 1955;54:980-984.
18. Kraus H. Clinical Treatment of Back and Neck Pain. New York, NY:McGraw-Hill; 1970.
19. Dommerholt J, Huijbregts P. Myofascial Trigger Points: Pathophysiology and Evidence-Informed Diagnosis and Management. Jones & Barlett Learning. 2009.
20. Baldry PE. Acupuncture, Trigger Points and Musculoskeletal Pain. Edinburgh, UK: Churchill Livingstone, 2005.
21. Wang H, Yu M, Ochani M, et al.Nicotinic acetylcholine receptor alpha7 subunit is an essential regulator of inflammation. Nature. 2003;421:384-8.
22. Tracey KJ. The inflammatory reflex. Nature. 2002;420:853-859.
23. van Maanen MA, Vervoordeldonk MJ, Tak PP. The cholinergic anti-inflammatory pathway: towards innovative treatment of rheumatoid arthritis. Nat Rev Rheumatol. 2009 Apr;5(4):229-32.
24. Tracey KJ. Physiology and immunology of the cholinergic antiinflammatory pathway. J Clin Invest. 2007;117(2):289-296.
25. Ulett GA, Han S. The Biology of Acupuncture. St Louis, MO:Warren H. Green; 2002.
26. Taub A. Nonsense with Needles. In Barrett S and Jarvis W. The Health Robbers: A Close Look at Quackery in America. Prometheus Books, Amherst, NY. 1993. Article available online at http://www.acuwatch.org/general/taub.shtml
27. Linde K, Streng A, Jurgens S, Hoppe A, Brinkhaus B, Witt C, Wagenpfeil S, Pfaffenrath V, Hammes MG, Weidenhammer W, Willich SN, Melchart D. Acupuncture for patients with migraine: A randomized controlled trial. JAMA 2005;293:2118-2125.
28. Melchart D, Streng A, Hoppe A, Brinkhaus B, Witt C, Wagenpfeil S, Pfaffenrath V, Hammes M, Hummelsberger J, Irnich D, Weidenhammer W, Willich SN, Linde K. Acupuncture in patients with tension-type headache: Randomised controlled trial. BMJ 2005;331(7513):376-382.
29. Scharf HP, Mansmann U, Streitberger K, Witte S, Kramer J, Maier C, Trampisch HJ, Victor N. Acupuncture and knee osteoarthritis: A three-armed randomized trial. Ann Intern Med 2006;145:12-20.
30. Campbell A. Point specificity of acupuncture in the light of recent clinical and imaging studies. Acupunct Med 2006;24(3):118-122.
31. Moffet HH. Sham acupuncture may be as efficacious as true acupuncture: a systematic review of clinical trials. J Altern Complement Med. 2009 Mar;15(3):213-6.
32. Moffet HH. Acupuncture trial lacks a priori rationale to refute null. hypothesis. Arch Intern Med. 2008 Mar 10;168(5):550-1.
33. Berman BM, Langevin HH, Witt CM, et al. Acupuncture for chronic low back pain. N Engl J Med 2010 Jul 29; 363(5):454-61.
34. Shanks LP. Flowers of Evil. Ives Washburn. New York, 1931.
![]()
What’s The Harm?
Any promoter of science-based medicine often faces the question – what’s the harm? What is the harm if people try treatment modalities that are not based upon good science, that are anecdotal, or provide only a placebo benefit? There are generally two premises to this question. The first is that most “alternative” placebo interventions are directly harmless. The second is that direct harm is the only type worth considering. Both of these premises are wrong.
The pages of SBM are filled with accounts of direct harm from unscientific treatments: argyria from colloidal silver, death from chelation therapy, infection or other complications from acupuncture, burns from ear candling, stroke from chiropractic neck manipulation – the list goes on. You can read anecdotal accounts of such harm on the website, whatstheharm.net. Of course, as we often point out, harm and risk is only one end of the equation – one must also consider benefit. It is the risk/benefit ratio of an intervention that is important. But generally we are talking about interventions that lack any evidence for benefit, and therefore any risk of harm is arguably unacceptable.
But perhaps the far greater harm comes from indirect causes. I was reminded of this with the publication of a study looking at flu vaccine uptake in 9 countries. They found that among older individuals who did not get the flu vaccine there was an increase in negative attitudes toward the vaccine, but also there was an increase in the use of traditional unscientific interventions. Cause and effect here is likely to be complicated. People who rely upon folk remedies may feel that they do not need the flu vaccine. Also, those who do not trust in the vaccine may then seek out alternatives. It is likely also true that the subculture of “alternative” medicine simultaneously fosters both a belief in unscientific treatments and a mistrust of mainstream science-based interventions.
The study authors conclude:
The hypothetical framework can be used to guide healthcare providers in developing strategies to foster normative beliefs of older people in vaccination, provide effective action cues and promote vaccine access.
“Normative beliefs” is a technical way of referring to the fact that promoters of “alternative” modalities tend to foster bizarre and unscientific beliefs in the public. Dubious treatments are often marketed with false notions about biology, physiology, and anatomy. It turns out, the iris of the eyes do not contain a functional map of the body (nor does the bottom of the foot). There is no human energy field or biofield or chi. Acupuncture points have not basis in reality. Magnets do not attract the iron in our blood. And toxins do not build up in our tissues, causes most diseases.
The consequences of fostering incorrect notions about human physiology and the nature of health and disease are difficult to measure or quantify, but they should not be ignored as a significant source of indirect harm from unscientific treatments.
The marketing of unscientific treatments often involves warning potential customers away from mainstream medicine, or at least downplaying the effectiveness of science-based treatments or overstating their risks. One does not have to look beyond any pro-CAM website to see articles scaring the public off science-based treatments side by side with advertisements for unscientific alternatives. The internet is unfortunately full of commercialized websites working directly against efforts to create “normative beliefs” in the public.
Belief in ineffective treatments and mistrust of science-based treatments may lead to delay in effective treatment and worse outcomes. In addition they create financial harm, which is increasingly important as health care costs rise. Financial harm can be extreme in cases of the desperation caused by serious illnesses. Tens of thousands of dollars are spent, for example, to send one patient to a fraudulent stem cell clinic. This financial harm is not limited to the patient or their family, as often such treatments are funded by charity from extended family, friends, and colleagues.
There is further psychological harm from creating false hope. I have personally seen the crushing effects such false hope can create when reality finally sets in. This can also significantly delay the process of psychologically dealing with a serious illness, which further affects important decision making about care. Wasting time of worthless treatments can also rob the terminally ill of precious time spent with loved-ones.
Further, the allure of unrealistic treatments diverts scarce resources (hospital space, research time and money) away from more fruitful modalities.
Conclusion
The ripple effect of harm that flows from unscientific medical beliefs is multifarious and significant, but often neglected by those who are not familiar with the phenomenon. “What’s the harm” is therefore a question we will have to answer frequently and for the foreseeable future.
![]()
Science and Morality
I have frequently said that science can only provide data to inform our decisions but can’t tell us what we “should” do; that it can determine facts but not values. I stand corrected. A persuasive new book by Sam Harris, The Moral Landscape, has convinced me that science can and should determine what is moral. In fact, it is a more reliable guide than any other option.

Several recent books have looked at morality from a scientific viewpoint. Animals have been shown to exercise altruism and to appreciate fairness. Human cooperation has been shown to offer a survival advantage to individuals and groups. Game theory has demonstrated the success of the tit-for-tat strategy. In The Science of Good and Evil, Michael Shermer argues that evolution has produced in us a moral sense that is not a reflection of some “absolute” morality but that constitutes a worthy human project that transcends individuals. He posits a pyramid of morality that becomes more advanced as it is applied to larger in-groups, from self to family to community to all living creatures. He amends the Golden Rule to specify that we should treat others not as we want to be treated but as others want to be treated.
Harris goes much further. With a background in both philosophy and neuroscience, he is qualified to do so. He points out that questions about values — about meaning, morality, and life’s larger purpose — are really questions about the well-being of conscious creatures. He says we know enough about the human brain and its relationship to events in the world to say that there are right and wrong answers to the most pressing questions of human life. He shows that it’s as senseless to claim morality is relative as to claim it is absolute. Morality cannot be understood as some Platonic ideal; it cannot be understood as whatever the preferred deity of one’s society has commanded; it cannot be dismissed as meaningless and varying with culture. Cultural relativism is stupid: we should never accept slavery or female genital mutilation as moral even in the societies that practice them believing they are moral. It is immoral and irrational to accept such practices out of political correctness and unwillingness to offend.
Harris has honed in on what we all believe, no matter what we might say we believe. He defines an action as moral if it increases the well-being of humans and other conscious beings, and immoral if it decreases well-being. We all accept that a good life is preferable to a life of suffering and that things like kindness to children are desirable. We all accept the Golden Rule: it’s not that we accept it because religion so dictates, it’s that religions have adopted it because we all know that it is valid.
Religion has long claimed that morality is its province, but this is clearly untenable. Different religions have different standards, religious commandments have encouraged immoral behaviors, non-religious societies are as moral as religious ones. Guidelines are inconsistent: the Catholic church excommunicates women who try to become priests, but fails to excommunicate priests who rape little boys. Religious morality also values human well-being, but with a difference. Most religions give priority to well-being in some imagined life after death. This often leads to unnecessary suffering in this, the only life we can be sure of.
Just as people are often wrong about science (i.e. rejecting evolution) people are often wrong about what is moral, but Harris sees signs of progress. Slavery is now universally condemned. Racism has diminished. But some societies mistreat women and deny them education, and our fear of offending the beliefs of others has prevented us from improving the lot of humanity by fighting certain clearly immoral practices. If morality can be established as a science, it will facilitate rational progress.
Science can have a great deal to say about morals. It can examine whether making women wear a burqa improves the well-being of a society. It can test whether corporal punishment has the beneficial results envisioned by those who prefer not to “spare the rod.” It can test whether abstinence-only education achieves its stated goal of reducing pre-marital sex. It can try to measure well-being. Well-being will be difficult to quantify, but not impossible. The environment and the individual’s response to it can be objectively studied. The important thing is to be willing to look at these issues and to try to evaluate moral questions through rational inquiry. It is no longer acceptable to claim that slavery would become moral if a society chose to practice it or to claim that homosexuality is an absolute evil.
It would be easy to reject Harris’ ideas as simplistic and impractical or to mistake hedonistic “happiness” for true well-being. If you think he is wrong, I would urge you to read the book to appreciate the subtleties and nuances of what he is actually saying.
Harris sees the moral landscape as one with valleys of suffering and peaks of well-being. He accepts that there can be different peaks with similar magnitudes, so there need not be one single prescription for all societies.
He sets us three ambitious projects:
- To explain why people tend to follow certain patterns of thought and behavior (many of them demonstrably silly and harmful) in the name of “morality.”
- To think more clearly about the nature of moral truth and determine which patterns of thought and behavior we should follow in the name of “morality.”
- To convince people who are committed to silly and harmful patterns of thought and behavior in the name of “morality” to break these commitments and to live better lives.
These may be phenomenally difficult, especially the third, but they are indisputably worthy goals to aim for. There must be something to know about meaning, morality and values in principle, if not always in practice. And Harris believes that merely admitting this will transform the way we think about happiness and the public good.
This is one of those books that can stretch the reader’s mind to new dimensions. Even the eminent Richard Dawkins was altered by reading it. He says,
I was one of those who had unthinkingly bought into the hectoring myth that science can say nothing about morals. The Moral Landscape has changed all that for me. Moral philosophers, too, will find their world exhilaratingly turned upside down, as they discover a need to learn some neuroscience. As for religion, and the preposterous idea that we need God to be good, nobody wields a sharper bayonet than Sam Harris.
![]()
Oprah’s buddy Dr. Christiane Northrup and breast thermography: The opportunistic promotion of quackery
As many readers know, October is Breast Cancer Awareness Month. What that generally means at our cancer center and in the rest of the “real world” is that, during the month of October, extra effort is made to try to raise awareness of breast cancer, to raise money for research, and promote screening for cancer. Unfortunately, what Breast Cancer Awareness Month means around the Science-Based Medicine blog is that a lot of breast cancer-related pseudoscience and outright quackery will be coming at us fast and furious. There’s no way, of course, that I can deal with it all, but there’s one area of medical pseudoscience related to breast cancer that I just realized that none of us has written about on SBM yet. Actually, it’s not really pseudoscience. At least, the specific technology isn’t. What is pseudoscience is the way it’s applied to breast cancer and in particular the way so many “alternative” medicine and “complementary and alternative medicine” (CAM) practitioners market this technology to women. The technology is breast thermography, and the claim is that it’s far better than mammography for the early detection of breast cancer, that it detects cancer far earlier.
I’ve actually been meaning to write about thermography, the dubious claims made for it with regard to breast cancer, and the even more dubious ways that it’s marketed to women. In retrospect, I can’t believe that I haven’t done so yet. The impetus that finally prodded me to get off my posterior and take this on came from what at the time was an unexpected place but in retrospect shouldn’t have been. You’ve met her before quite recently when SBM partner in crime Peter Lipson took her apart for parroting anti-vaccine views and even citing as one of her sources anti-vaccine activist Sherri Tenpenny. I’m referring, unfortunately, to one of Oprah Winfrey’s stable of dubious doctors, Dr. Christiane Northrup. Sadly, Peter’s example of her promotion of vaccine pseudoscience is not the first time we at SBM have caught Dr. Northrup espousing anti-vaccine views. We’ve also harshly criticized her for her promotion of “bioidentical hormones” and various dubious thyroid treatments. However, Dr. Northrup is perhaps most (in)famous for her advocating on Oprah’s show the use of Qi Gong to direct qi to the vagina, there apparently to cure all manner of female ills and promote fantastic orgasms in the process. This little incident ought to tell you nearly all that you need to know about her. Even Oprah looked rather embarrassed in the video in which Dr. Northrup led her audience in directing all that qi goodness “down below.”
What brought Dr. Northrup to my attention again was my having joined her e-mail list. As you might imagine, I’m on a lot of e-mail lists, ranging from that of Mike Adams, to Generation Rescue, to Joe Mercola and beyond. I do it all for you, in order to have the blogging material come to me rather than my having to seek it out. True, the price is that my e-mail in box is frequently clogged with quackery, but it’s a small price to pay. This time around, Dr. Northrup’s e-mail brought my attention to a post of hers, Best Breast Test: The Promise of Thermography. It was truly painful to read, and I consider it inexcusable that someone who claims to be an advocate of “women’s health” could write something that reveals such ignorance. But, then, I suppose I shouldn’t be surprised after her recent flirtation with anti-vaccine views. If it isn’t already complete, Dr. Northrup’s journey to the Dark Side is damned close to complete. You’ll see what I mean right from her very introduction:
Every year when Breast Cancer Awareness Month (October) comes around I am saddened and surprised that thermography hasn’t become more popular. Part of this is my mindset. I’d rather focus on breast health and ways to prevent breast cancer at the cellular level than put the emphasis on testing and retesting until you finally do find something to poke, prod, cut out, or radiate.
Let me take a moment to note the framing that Northrup uses. She’s all about “prevention,” or, at least, that’s what she wants you to think she’s all about. This is no doubt meant to be a stark contrast to us reductionistic, “Western,” “allopathic” physicians who, according to typical “alt-med” tropes, don’t give a rodent’s posterior about prevention but only care about, as Northrup so quaintly put it, “poking,” “prodding,” “cutting out,” and “irradiating.” The only alt-med trope Northrup left out of her attempt to don the mantle of prevention is “poisoning.” (I suppose I should be thankful that she managed to restrain herself that much.) But what does it mean to “prevent breast cancer at the cellular level”? That’s just a scientifically empty and meaningless buzz phrase, especially coming from her.
How would thermography achieve “prevention at the cellular level”, anyway? Thermography is just another test. In intent the use of thermography is no different than mammography in that its advocates claim that thermography can find breast cancers at an early stage. Its advocates also use thermography in damned close to exactly the same way that we use mammography. They use the test on asymptomatic women periodically to try to detect cancer early. There’s zero “prevention” involved. Even if thermography worked as well as its proponents (like Dr. Northrup) claim, there would still be zero prevention involved. Northrup’s use of the term “prevent breast cancer at the cellular level” is as empty as her head is apparently of knowledge about breast cancer and as empty as her handwaving about thermography.
Yes, it’s utter nonsense, but Dr. Northrup’s blather does echo many of the claims made for thermography. For instance, if you go to BreastThermography.com, a site that is clearly pro-thermography, you’ll find a whole bunch of similar claims, such as that thermography detects cancer earlier, that it can provide an “individualized breast cancer risk assessment,” that it’s better for younger women, and that it can detect “thermal signs of hormone effects” that can be used for breast cancer prevention. It ends up including the groundless recommendation that “every woman should include breast thermography as part of her regular breast heath care.” Pointing out that the “incidence of breast cancer is on the rise” (it isn’t, by the way, and hasn’t been for years; in fact, it’s decreasing), the website then makes the completely baseless recommendations that every woman should have a baseline scan at age 20 and then be scanned every three years between ages 20-30 and every year after age 30.
BreastThermography.com also has a quack Miranda warning on its front page:
Disclaimer: Breast thermography offers women information that no other procedure can provide. However, breast thermography is not a replacement for or alternative to mammography or any other form of breast imaging. Breast thermography is meant to be used in addition to mammography and other tests or procedures. Breast thermography and mammography are complementary procedures, one test does not replace the other. All thermography reports are meant to identify thermal emissions that suggest potential risk markers only and do not in any way suggest diagnosis and/or treatment. Studies show that the earliest detection is realized when multiple tests are used together. This multimodal approach includes breast self-examinations, physical breast exams by a doctor, mammography, ultrasound, MRI, thermography, and other tests that may be ordered by your doctor.
All of which would be fine as far as it goes, except that thermography shouldn’t be considered anything more than an experimental technique and the above paragraph does not describe how Northrup is promoting thermography.

Thermography: The Data
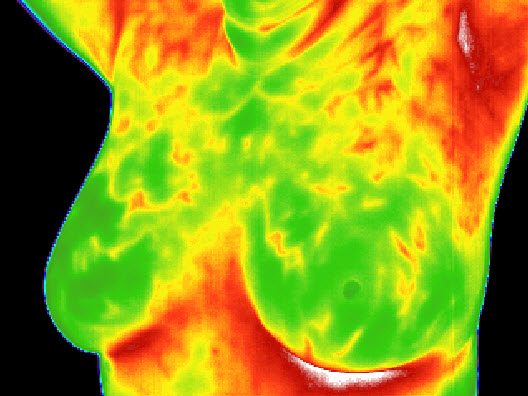
What is thermography and how is it used to detect breast cancer? As its name implies, thermography measures differences in temperature. Most systems use infrared imaging to achieve these measurements. There’s nothing magical about it; the technology has been in use for various applications for decades. The rationale for applying thermography to the detection of breast cancer is that breast cancers tend to induce angiogenesis, which is nothing more than the ingrowth of new blood vessels into the tumor to supply its nutrient and oxygen needs. A tumor that can’t induce angiogenesis can’t grow beyond the diffusion limit in aqueous solution, which is less than 1 mm in diameter. These blood vessels result in additional blood flow, which results in additional heat. In addition, the metabolism of breast cancer cells tends to be faster than the surrounding tissue, and cancer is often associated with inflammation, two more reasons why the temperature of breast cancers might be higher than the surrounding normal breast tissue and therefore potentially imageable using infrared thermography.
Although thermography is scientifically plausible, unfortunately its reality has not lived up to its promise, Dr. Northrup’s claims notwithstanding. Let’s take a look at those claims:
I understand that mammography has been the gold standard for years. Doctors are the most familiar with this test, and many believe that a mammogram is the best test for detecting breast cancer early. But it’s not. Studies show that a thermogram identifies precancerous or cancerous cells earlier, produces unambiguous results (which cuts down on additional testing), and doesn’t hurt the body.
No, studies do not show anything of the sort, other than that thermography probably doesn’t hurt the body. In particular thermography does not produce unambiguous results—far from it! That’s the problem, and that’s the reason why thermography has not caught on. It’s unreliable, and it doesn’t provide much in the way of anatomic information that allows a better localization of the breast cancers it does find. You’ll note if you look at Dr. Northrup’s article that the most recent article she cites that directly addresses the use of thermography to detect breast cancer is from 1982. There are more recent reviews and studies, as you might expect, but, oddly enough, Dr. Northrup doesn’t cite them.
One aspect of thermography for breast cancer detection that its advocates almost always mention is that it is FDA-approved for the detection of breast cancer. That is true, but not in the way it is often implied. Yes, thermography is FDA-approved for the detection of breast cancer, but what they don’t tell you is that thermography is not approved alone for screening women for the detection of breast cancer. It’s approved to be used in conjunction with mammography. What thermography boosters also fail to tell you is that the reason why thermography fell out of favor 30 years ago was as a result of a study by Feig et al in 1977 that found thermograpy to come in dead last among existing screening modalities of the time in finding breast cancers. Mammography detected 78% of breast cancers. In contrast, thermography only detected 39%, and in all 16,000 women in the study thermography was interpreted as positive in 17.9%. This is not a stellar record. In a separate trial in the early 1970s, the Breast Cancer Detection Demonstration Project (BCDDP) planned to compare thermography, mammography and clinical examination. However, BCDDP investigators decided to drop thermography early in the project due to a high false positive rate and low sensitivity.
Of course, technology was a lot more primitive back then, both in its ability to detect differences in temperature and its ability to produce images; it’s not at all surprising that thermography would not perform as well. Add to that the problems of bulky equipment, some of which required liquid nitrogen to work, and the lack of computational power to analyze images, and it’s not surprising that, compared to mammography, thermography never really caught on. Indeed, in a 1985 review, Moskowitz analyzed the data from the BCDDP trial. Of the 1,260 patients with more than one positive thermogram from 1973 to 1976, 1.9% subsequently developed breast cancer from 1977 to 1983. That finding was not statistically significantly different from the 1.3% of patients who developed cancer and never had a positive thermogram. His review of the literature supported the dismal record of thermography for detecting breast cancer.
That was 30 years ago, though. What about now? Computing power has increased almost ridiculously since then, and newer thermal sensors can detect temperature differences of 0.08° C. Has technology evolved to the point where the shortcomings of the original studies that buried thermography as a viable competitor to mammography for breast cancer screening no longer apply?
Maybe. Maybe not. That’s exactly the problem. As pointed out by Gregory Plotnikoff, M.D., M.T.S., and Carolyn Torkelson, M.D., M.S. in a 2009 commentary in Minnesota Medicine entitled Emerging Controversies in Breast Imaging: Is There a Place for Thermography?:
The biggest question concerns the efficacy of thermography to detect breast cancer. Despite various studies that suggest positive results for thermography, there has never been a major randomized controlled trial to determine baseline measurements of sensitivity and specificity. It is hard to imagine thermography being accepted by the conventional medical establishment without such data or evidence of cost-effectiveness.17 In addition to questions about the effectiveness of thermography, research needs to be conducted to determine the cost of using it for widespread cancer screening.18
Even two naturopaths reviewing the thermography literature in 2009 in one of the most woo-friendly journals imaginable, Integrative Cancer Therapies, conclude:
In light of developments in computer technology, and the maturation of the thermographic industry, additional research is required to confirm and/or continue to develop the potential of this technology to provide effective noninvasive early detection of breast cancer.
Even though the naturopaths tried very hard to spin the data into as favorable a view as possible, they just couldn’t bring themselves to recommend routine thermography. Meanwhile, virtually every reputable professional organization whose purview includes breast imaging and breast cancer does not recommend it. Here is a typical position statement, this time from cancer organizations in New Zealand.
That’s not to say that there aren’t “positive” trials of thermography. The problem is that they don’t rise to the level necessary to justify recommending thermography to all women, as many of these chiropractors and naturopaths are doing. There was a recent study of 92 women in 2008 that, using a technology called Digital infrared thermal imaging (DITI), found a sensitivity of 96% and a specificity ranging between 12-44%, depending upon the setting of the machine. While this is promising, it’s not possible to justify the widespread use of this technology on the basis of such a small clinical trial. One also has to remember that thermography also has downsides relative to mammography. For example, women have to let their skin temperature equilibrate to the room temperature of the thermography suite by sitting naked from the waist up in the dressing room for 15 minutes before the examination can be done:
For the scan, the patient is asked to stand about 10 feet in front of the camera with her arms raised over her head while three views of the breast (anterior and two lateral views) are taken. The next step in the process is a “cold challenge” where the patient is asked to place both hands in cold water at 10°C for one minute; then these same three images are retaken.43,44 The breasts exhibit thermal patterns that are captured by the infrared camera. It is these thermal captured image patterns that are interpreted by a trained thermographer.
Other protocols I’ve read about include blowing cool air on the breasts to speed the equilibration.
There is also considerable opportunity for subjectivity in the interpretation of thermograms. This is because, in marked contrast to mammography, there aren’t any widely agreed-upon standards for the performance and interpretation of breast thermography. Plotnikoff and Torkelson described the state of the industry quite well, with one huge blind spot:
In its current state in the United States, thermography is a balkanized industry. Although thermography never took root in mainstream medicine, it has begun to flourish in alternative settings as a breast cancer detection service offered by some physicians, chiropractors, and naturopaths. In lieu of any industry or professional standards for thermography, a variety of practices and protocols have emerged among practitioners and equipment manufacturers. As one practitioner described it, the industry is in its “Wild West” days.19 This fragmented state weakens the credibility of the entire field because consumers have no way to distinguish credible from inferior thermographic techniques. As thermography emerges as an alternative screening tool, consumers are led to believe that it has been validated for efficacy and compared with mammography. This misconception could raise public-safety concerns.
“Misconception”? Have Plotnikoff and Torkelson been reading the ads for breast thermography on the web? These go far beyond simply claiming that thermography has been validated for efficacy and compared with mammography.

The marketing of thermography by CAM practitioners
Thermography has become very popular among chiropractors, homeopaths, naturopaths, and a wide variety of “alternative practitioners.” Indeed, many are the ads that claim that thermography is safer than mammography and that it can replace mammography for breast cancer screening, particularly for younger women. Typical of such marketing and propaganda is this article by Joe Mercola entitled Revolutionary and Safe Diagnostic Tool Detects Hidden Inflammation: Thermography as a means of marketing the test at Dr. Mercola’s Natural Health Center in the Chicago area:
In this ad, Mercola claims that mammograms cause breast cancer, that the compression used during mammography can lead to “a lethal spread of any existing malignant cells,” and that thermograpy can identify inflammation that leads to cancer that can be treated—all using diet and Mercola’s supplements, of course—to prevent breast cancer. He also claims that thermography is good for more than just breast cancer detection. If you believe Mercola, it can also detect a whole panoply of conditions, including arthritis, immune dysfunction, fibromyalgia, carpal tunnel syndrome, irritable bowel syndrome, diverticulitis, and Crohn’s disease.
Geez, is there anything thermography can’t do?
Well, if we’re to believe Dr. Northrup, this is another thing breast thermography can do:
The most promising aspect of thermography is its ability to spot anomalies years before mammography. Using the same ten-year study data,2 researcher Dr. Getson adds, “Since thermal imaging detects changes at the cellular level, studies suggest that this test can detect activity eight to ten years before any other test. This makes it unique in that it affords us the opportunity to view changes before the actual formation of the tumor. Studies have shown that by the time a tumor has grown to sufficient size to be detectable by physical examination or mammography, it has in fact been growing for about seven years achieving more than twenty-five doublings of the malignant cell colony. At 90 days there are two cells, at one year there are16 cells, and at five years there are 1,048,576 cells—an amount that is still undetectable by a mammogram. (At 8 years, there are almost 4 billion cells.)”
Of course, even if this were true (and no evidence is presented to show that it is), as I’ve pointed out time and time again, ever earlier detection of cancer is not always a good thing because not all early lesions progress to become cancer. In other words, detecting breast cancer earlier is in general a good thing most of the time, but there clearly exists a point of diminishing returns and a point beyond which detection that is too early has the potential to cause harm. The very issue in the recent rethinking of recommendations for mammography (most recently discussed just two weeks ago) hasn’t been that mammography is not sensitive enough, but rather its potential to detect too many breast cancers that would never progress to endanger the life of the woman.
Let’s put it this way. Even if everything Northrup says or cites is absolutely accurate and thermography can detect inflammatory states that lead to cancer several years before mammography, that would not necessarily save even a single life but would have the potential to cause even more harm through overdiagnosis and overtreatment, particularly given that as many as one in five mammographically detected breast cancers might never progress—and some might even regress. Detecting such lesions five to ten years earlier could only exacerbate the problem of overdiagnosis and overtreatment. It might also lead to the perfect situation for CAM practitioners. They could find breast “lesions” with thermography; prescribe “treatments” in the form of dietary manipulations, supplements, or whatever; watch the lesions either disappear spontaneously or not progress; and then claim credit for having “cured” or “stopped the progression of” the cancer. Even if the cancer progresses to where it requires surgical removal and other treatment, the quack can claim credit for having detected it “before mammography.”
If you want evidence that Dr. Northrup has truly gone completely woo, look no further than this next passage:
As with anything, I suggest you let your inner guidance help you in all decisions about your health. If you feel it’s best to get an annual mammogram, then by all means continue with them. Just be aware of the drawbacks and risks associated with the test. One helpful way to assess your risk for breast cancer—which in turn can help you decide how often you want to have mammograms—is to use the National Cancer Institute’s Breast Cancer Risk Assessment Tool, available online at http://www.cancer.gov/bcrisktool. After you answer seven simple questions, it calculates both your risk of getting invasive breast cancer in the next ?ve years as well as your lifetime risk, and it compares each to the risk for the average U.S. woman of the same age and race or ethnicity.
You would be surprised by how many women tell me their doctors make them feel guilty for not having a mammogram. Women who just know they have healthy breasts. Don’t be intimidated if you prefer to forgo annual mammography.
If Dr. Northrup truly tells her patients that it’s medically acceptable for them to forego mammograms and use thermography instead for their routine screening for breast cancer, she is guilty of gross malpractice, in my opinion. If she doesn’t tell her patients that but writes articles like the one I’m citing, she’s guilty of hypocrisy. Her statements are scientifically unjustified, profoundly unethical, and potentially dangerous to patients. Many are the women whom I’ve met who “just knew” they were fine until their family persuaded them to undergo mammography, which then found real, invasive cancers. I don’t have much faith in anyone’s “inner guidance” with regard to asymptomatic disease. In essence, Northrup is urging women to base their health care decisions on intuition rather than science.
The bottom line
Thermography is a technology that has some degree of scientific plausibility but has not been validated as a diagnostic modality to detect breast cancer. The studies from 30 years ago showed it to be markedly inferior to mammography for this purpose, the claims of naturopaths, chiropractors, and various other quacks notwithstanding. While it’s true that advances in technology and computing power might have brought thermography to a point where it might be a useful adjunct to current imaging techniques, large randomized clinical trials have not been done to define its sensitivity and specificity and determine its utility when added to routine mammographic screening. In addition, thermography doesn’t provide any information that breast MRI can’t provide—and provide better. MRI measures in essence the same thing that thermography does (blood flow, which is what the heat maps that thermography produces are surrogates for) and adds to it detailed anatomic information that can guide biopsy and excision. That’s something thermography can’t do.
Currently, my take is that thermography might be useful as an adjunct to mammography. Indeed, I’ll make a confession. Back when I worked at The Cancer Institute of New Jersey, I became involved with a project that was testing a thermography-like machine. (I can’t say more than that about it.) A startup company was testing its new device to determine if the combination of mammography plus this technique could improve the sensitivity and specificity of breast cancer detection. I don’t know what ever became of the company or the device, but I still view thermography basically the same way now as I did then. It’s a test that might be useful as an adjunct to mammographic screening. In order to determine whether thermography is useful as an adjunct to other imaging techniques, however, its proponents need to do the proper scientific validation and clinical testing first, which haven’t been done yet and will require large clinical trials. Until that testing is done, thermography should not be offered to women outside of a clinical trial, and it should never be offered to women in lieu of mammography to detect breast cancer. Science does not support the former indication, although I have to concede that it might one day. More importantly, science most definitely does not support the use of thermography instead of mammography, a use that I doubt any clinical trial is likely ever to support because clinical equipoise demands that thermography be added to mammography in any clinical trial, not tested instead of mammography.
The ironic and sad thing about thermography is that it is not per se quackery itself. The concept of breast thermography is based on a reasonable and scientifically plausible idea, namely that tumors produce more angiogenesis, which leads to more blood flow, which leads to more heat that can be detected and imaged. However, the way it is marketed and promoted as a replacement for mammography is quackery, and Dr. Northrup is buying into such highly dubious promotion, coupled with a condescending appeal to “women’s intuition.” Unfortunately, the tight embrace of quacks to thermography contributes to the unsavory reputation the technique currently has in the medical community and continues to hinder its development in mainstream scientific medicine. On the other hand, maybe the quacks like it that way. If mainstream medicine were ever to validate thermography scientifically, then it would become science-based medicine, and the quacks can’t have that. It’s too profitable to market the test through fear and misinformation.
![]()
Reflexology. Insert Nancy Sinatra Reference Here.
In the last post on acupuncture, I noted that the University of Maryland offered reflexology along with other supplements, and complementary and alternative medicine (SCAMs). I was uncertain as to the particulars of this SCAM, and this post is a result of those investigations.
Although messy in reality, science is a tool that gives us an idea as to how the real world functions. People will observe some aspect of nature, often for a lifetime, and from those observations discover a pattern in the data. Tycho Brahe spent a life carefully measuring the orbits of the planets; the data was used later by Kepler to determine that the planets orbit in an ellipse with the sun at one of the foci. If you have knowledge of the history of science, you realize what an amazing feat this represents, both in the measurement of the orbits and the analysis of the data. Careful observation, analysis of the data, then conclusions.
This is in contrast to SCAMs, where so many of the interventions are discovered by revelation, and then developed independently of data and observation. Palmer and chiropractic, von Peczely and iridology, Usui and reiki are examples. These geniuses discovered aspects of existence unseen by anyone before or after.
In that time honored pantheon is Dr. William Fitzgerald who, at the turn of the last century, “discovered” that the human body is divided into 10 longitudinal energy zones that end in the hands and the feet. By massaging these zones, you could heal disease and alter bodily functions. These are reminiscent of the meridians of acupuncture, and will soon be illustrated in the New England Journal of Medicine (see posts Aug 4 and 13). Fitzgerald named it Zone Therapy, and it went by that name until the 1960’s, when Eunice Ingham decided that, since all the energy zones ended in the feet, that it was the terminus of the energy zones that was the important aspect of Zone Therapy.
The body, it turns out, is far more crowded that we could ever have expected from our understanding of gross anatomy and histology. There is so much packed into our bag of meat, I am surprised that we do not explode, although perhaps we do have a potential explanation for spontaneous human combustion: the friction of all the projections and energy channels described by various SCAM’s rubbing together in a tight space.
There is the map projected on the iris with iridology, the maps on the ear, the tongue, the head, the hand, and the feet of the various acupuncture styles. There are the meridians of acupuncture and zone therapy, the energy flows of reiki and chiropractic. And there is the map of the body projected onto the feet and hands by reflexologists. The feet must be particularly crowded as the maps for foot acupuncture are different than the maps for reflexology; no wonder my feet ache at the end of the day.
Reflexologists are of the opinion that by manipulating the feet, hands and/or ears that correspond to body parts they can induce changes in those body parts. Touch the liver zone on the foot, alter the liver in the abdomen. Alexander Pushkin could vouch for the veracity of a subset of those interventions. Others are of the opinion that the manipulation of the feet, hands and/or ears alters the qi balance in the patient. However, as the Reflexology Association of American notes, “no one definition that will work in all situations and yet, because of the multi dimensional affect [sic] of Reflexology, all are true at [sic] defining the work we do. ”
And it is true, these definitions are limiting, as they do not encompass … well, let’s be nice and call them the curious concepts describing reflexology:
The purpose of the nerves is to carry messages and instruct the body. When the nerves improve that instruct the body, the instruction has to improve, the body has to improve. Every nerve in the body begins and ends in the hands and feet. By applying this specialized exercise pressure on the foot, the outcome is improved instruction to each and every part of the body, resulting in a re-educating, a re-patterning, and a re-conditioning of the nerves& instruction through the reflex/neutral electrical system of the body…also every lymphatic vessel begins and ends in the hands and feet.
The hands and feet are crowded indeed. Safe to say that the basic premises of reflexology have no bearing in reality. There are not projections of the body onto the hands and feet. As I have mentioned in the past, when I was a child I thought the Broadway in Portland was the same Broadway in New York and that if I kept walking I would end up on the Great White Way. It is true, in a way, that the two Broadways are connected in the same way that the nerves in the foot are connected to the liver, but it takes more links to get from one to the other than to get to Kevin Bacon.
What can reflexologist treat? Near about anything; it depends only on the claim of the reflexologist. Like many SCAMs, reflexology can help all illnesses. I would not deny that it is relaxing and pleasant to have one’s feet massaged — er, reflexed? (Reflexologist emphasize they are not doing massage.) But does reflexology have any real effects on any pathological states? Besides sore feet? And, while we are on the topic, why doesn’t walking have the same effect as reflexology?
Reflexology has been tested in clinical trials. Here is an issue that really gripes my cookies, or maybe a severe case of jealousy re: alt med.
In the world of infectious disease, getting to test an intervention for human use is a long process. First they have to find a potential antibiotic, discover the chemical structure and mechanism of action. Then the antibiotic is tested against numerous strains of hundreds of pathogens to see if it works in the test tube. Then there are a variety of animal studies looking for safety and efficacy. Then graduated clinical trials, phase 1, phase 2, and, finally, phase 3, before the antibiotic is declared non-inferior to vancomycin in human soft tissue infection.
Reflexology, and all other alt med interventions, bypass all these steps and go straight to clinical trials. Someone can pull a therapeutic intervention out of, well, this is the SBM blog, let’s say thin air, yeah, thin air. They can pull an intervention out of thin air and the next thing you know, good money is being spent to see if it is effective, when, evaluating it on the basis of reality, it should have the same chance of being effective as more common substances found in, well, ‘thin air.’
So, ignoring the fact there is no reason to test the efficacy of reflexology, what has reflexology been found to be effective in treating? Almost nothing of note. It is not effective for post operative cortisol levels, head ache, asthma, post operative pain, cancer anxiety, irritable bowel syndrome, pregnancy edema, low back pain, ovulation, and multiple sclerosis. It seemed to help pre-menstrual syndrome — so says the abstract which, I’m sure, accurately represents an unbiased and flawless experiment — but it did not even seem to help menopause symptoms.
What a hodgepodge of diseases. I thought aspirin was the wonder drug that worked wonders. The alleged near universality of reflexology, and other alt med interventions, is staggering. Imagine an antibiotic that not only treated all viruses, bacteria, fungi, and parasites but also infertility, headache, dementia and post op pain. Only alternative interventions have that kind of power. I am stuck looking for the underlying cause of a disease and targeting it with a specific intervention. How Western and reductionist of me.
While almost all individual studies show no benefit of reflexology, what would a systematic review reveal? The summation of nonsense, unfortunately, does not lead to validation of reflexology. Put all the small piles of nonsense together, you get one big pile of nonsense. The studies of reflexology are poorly done, with small sample size, and, not mentioned in the review, had no reason to be done in the first place.
Studies in breast cancer patients suggest to me that human contact is what it important, not the specific modality.
PATIENTS AND METHODS: One hundred and eighty-three women were randomized 6 weeks post-breast surgery to self-initiated support (SIS) (comparator intervention), SIS plus reflexology, or SIS plus scalp massage (control for physical and social contact). Reflexology and massage comprised eight sessions at weekly intervals. The primary end-point was 18 weeks post surgery; the primary outcome measure was the Trial Outcome Index (TOI) of the Functional Assessment of Cancer Therapy (FACT-B) – breast cancer version. The secondary end-point was 24 weeks post surgery. Secondary outcome measures were the Hospital Anxiety and Depression Scale (HADS) and the Mood Rating Scale (MRS).
RESULTS: At primary end-point, massage, but not reflexology, was significantly better than SIS on the TOI. Reflexology and massage were both better than SIS for MRS relaxation. Massage was better than reflexology and SIS for MRS easygoingness. At secondary end-point, reflexology, but not massage, was better than SIS on the TOI and MRS relaxation. There were no significant differences between reflexology or massage. There were no significant between group differences in HADS anxiety and depression. Self-reported use of out of study complementary therapies indicated that this was unlikely to have a significant effect on findings.
Or this one:
…significant decrease in anxiety observed in this sample of patients with breast and lung cancer following foot reflexology suggests that this may be a self-care approach to decrease anxiety in this patient population.
Or in the demented:
The findings demonstrate that when receiving the reflexology treatment condition, as compared to the control condition, the residents demonstrated significant reduction in observed pain.
All groups whose underlying disease leads to less human contact. Have you hugged your demented, cancerous nursing home patient today? I didn’t think so.
Monkeys, and other animals, groom each other often with a marked reduction in stress. Touch is good, and one doesn’t need to wrap it up in pseudoscientific nonsense for it to beneficial. Well, maybe you do. Strange people offering to massage your feet because it feels good may be off-putting for some and could lead to the authorities being involved.
One doesn’t need the woo of reflexology (projected maps and altered qi) to recognize that people need and benefit from physical interactions. Like in the NEJM recently, demonstrating the tai chi was of benefit in fibromyalgia. Exercise helps fibromyalgia, and tai chi is a gentle form of exercise, so it’s no surprise tai chi was of benefit; so is yoga. The mystical magic adds nothing.
Oddly, no one seems to have tested reflexology as an intervention for foot pain, a common complaint, and reflexology could not decrease foot edema in pregnant females. One wonders, if reflexology can’t even help a foot problem, what good is it?
The irritable bowel syndrome study concludes
I want to conclude with a note of caution. Although the results of this study are quite clear, they should not be used to dismiss reflexology as a treatment option across the board, nor indeed to argue against the effectiveness of CAM as a whole. The simple fact is that we know very little about the effectiveness of very many treatment options in relation to very many conditions. Reflexology in particular remains not just under-researched but almost unresearched, something that is quite startling given the extent of its use.
This is somewhat mirrored in the systemic review:
…the paucity and the poor quality of the existing studies prevents definitive judgement about the value of reflexology.
Well, technically, that’s true. But there is more than sufficient understanding about the workings of the human body to render a definitive judgement on reflexology. It won’t work because it can’t work, in much the same way that we know that a perpetual motion machine won’t work because it can’t work. And yet people keep inventing perpetual motion machines. Just because the rules of the universe say something is impossible doesn’t stop them from trying.
The great majority of studies demonstrate reflexology had no effects that could not be replicated by beyond picking fleas off your mate (am I over sharing?). And it has no anatomic or physiologic justification.
Years ago I was at a conference and one of my attendings was being detailed about a new antibiotic. The rep concluded with “and it’s very popular in Europe” to which my attending responded “so was fascism” and strolled off. Popularity is not a good justification to spending money and wasting patient’s limited time with nonsense.
![]()
Pat Schroeder’s endorsement of Rage Reduction Therapy: The Cult of the Celebrity Strikes Again
We all know that misguided celebrities, such as Jenny McCarthy, Oprah, Prince Charles, and Arianna Huffington, pose considerable public health threats. Few know that arguably the most vile form of quackery has been getting the thumbs up from a celebrity hailing from the most rarified heights of power and influence — Representative Patricia Schroeder (D-CO, 1973-1997).
The practice I’m referring to is “Rage Reduction.” This practice, popular for decades in adoption and foster care circles, claims to help children develop the capacity to love and become attached to their new caregivers. Practitioners believe these children suffer from “Attachment Disorder” because of early abuse and neglect. Typical of quackery, this unrecognized diagnosis consists of an absurdly long catch-all list of signs used to ensnare any child. (Even good behavior is interpreted as sneaky manipulation of parents.)
In a Rage Reduction therapy session, a child is restrained by a therapist – usually a licensed psychologist or social worker – plus one or more assistants. The therapist “activates” a child by yelling, belittling, threatening, relentlessly tickling, bouncing the child’s head, covering his mouth, and painfully knuckling the child’s rib cage and sternum. Such sessions typically go on for two or more hours, until the child is exhausted from struggling and becomes, as one psychologist observed, “a whimpering little puddle.” Children, even teenagers, are then swaddled and given a baby bottle by their adopted mother for “bonding time.”
The rationale for Rage Reduction consists of several thoroughly discredited notions: the need to regress children back to infancy so that “repressed” memories of abuse can be recovered and repressed “infantile anger” can be drained out through “catharsis.”
There is no reliable evidence that indicates that Rage Reduction would be anything but harmful. To critics, Rage Reduction is indistinguishable from literal torture, i.e. the infliction of severe pain or suffering, whether physical or mental, for a purpose. The purpose here is apparently not the creation of loving relationships, but rather grinding down children until they are grateful and unquestioningly obedient. Think “Stepford Children.”
In one particularly brutal form of Rage Reduction called “Compression Therapy,” therapists claim to provoke repressed memories of rape by lying on top of the child and licking the child’s face. Along with violating just about every ethical code in the mental health book, Compression Therapy puts much pressure on the child’s abdomen, making breathing difficult. At least two children have died from suffocation in Rage Reduction sessions; and survivors tell of “seeing stars,” and even of passing out during therapy.
Many criminal child abuse and death cases have been linked to Rage Reduction and its harsh parenting methods. For those with a strong stomach, there is a blogsite that has published several survivor accounts.
Rage Reduction got its start in Colorado back in the 1970s, when psychologist Robert Zaslow came to the state claiming he could cure blindness. Zaslow had served as consultant on Elvis Presley’s last movie, A Change of Habit (1969). In this film, “Dr.” Elvis cures a girl of autism in just one Rage Reduction session.
When Rage Reduction failed to cure blindness, or autism off screen, Colorado followers of Zaslow turned to treating “attachment breaks” in children. The practice really took off in the late 1980s when adoptions from Eastern Europe opened up – and when Rage Reduction got a big celebrity bump from none other than US Representative Patricia Schroeder.
Schroeder was the long-time Democrat Congresswoman representing the Denver area who took a stab at the presidency in 1988. Chairing the US House Select Committee on Children, Youth and Families, Schroeder billed herself as “Friend of the Family.”
At the peak of her influence, Schroeder also wrote the foreword for a book promoting Rage Reduction entitled High Risk: Children Without A Conscience by Ken Magid and Carole McKelvey (Bantam, 1987). Today, after one author has surrendered her therapy license (the other is dead), this book is still in print.

US News & World Report later took note of Schroeder’s “promotion” of High Risk:
High Risk has a foreword by former Colorado Rep. Pat Schroeder, who thanks the authors for their “gift” at a time when inadequate day care, rising divorce rates, and teen pregnancy threaten to inflate the numbers of unattached kids.
“A Dead Child, A Troubling Defense” by Miriam Horn)
Shortly after High Risk was published, HBO aired a documentary about a child being treated by Magid. This film, Child of Rage, was followed up with an HBO drama by the same name. Both films, like the book, portrayed “unattached” children as murderous psychopaths, a danger to parents and society at large. This sensationalism fueled Rage Reduction ascendancy into a fad therapy, with cult-like followings all over the country, and in Britain and Australia, as well. Without Schroeder’s endorsement, Rage Reduction might have otherwise died a quick death — from lack of research, from moral outrage, and from compassion for children.
Today, High Risk is considered by critics to be the worst book of its kind. If a therapist recommends High Risk, you’ve pretty much got him pegged as an adherent of coercive restraint therapies. No one else would likely want to be associated with it.
High Risk contains one photo that nearly says it all. It is a photo of psychiatrist Foster Cline, MD knuckling the sternum of a young boy.

The caption says:
Dr. Foster Cline illustrates how a Rage Reduction Therapy session is conducted….Cline stimulates subject toward rage reaction. Child is being held by “holders.” …[the] child screams how much he hates the therapist.
When a boy with a bruised chest escaped Cline’s center a few years later, Cline was ordered by the Colorado Board of Medical Examiners to stop using Rage Reduction. Cline opted to leave the state instead.
This extreme treatment, which High Risk likens to an “exorcism,” is justified by demonizing children with “Attachment Disorder.” The same US New & World Report article explains:
A cartoon in the book Schroeder promotes depicts a spectrum of well-being: from the securely attached like “Mother Teresa,” illustrated with a haloed saint holding a cross, to the severely unattached like “Charles Manson,” depicted as a horned devil holding a bloody knife. Paula Pickle says of the kids her center [Attachment Center at Evergreen, Colorado] treats that “there often doesn’t seem to be a heart or soul.” [Thais] Tepper [of Parents' Network for the Post-Institutionalized Child] explains in chilling terms the effort by Russian orphanages to get rid of their most troubled charges: “Who are you going to send abroad, the healthy kids or the little minions of Satan?”


The banality of this diagram is almost unworthy of being pseudoscience. It’s not junk science. It’s just plain junk. (But do note, Ms Schroeder, where “Some Politicians” rank on this scale.)
High Risk does dabbles in other pseudoscience, as well, e.g.:
What Ted Bundy’s Handwriting Reveals..His manipulative tendencies are indicated by the “hooks” in some of his “c’s.”
Rage Reduction, repackaged with the less explicit name of “Attachment Therapy,” flourished through the 1990s. A welter of child welfare workers, CASA volunteers, judges, and adoptive/foster parents were sucked into the pseudoscientific solutions offered by Attachment Therapy.
With Schroeder’s imprimatur firmly in place, government agencies at federal, state and local levels funneled money into Attachment Therapy, paying for treatment and to house children in special “therapeutic foster homes” versed in Attachment Therapy’s uber harsh parenting methods, aka Nancy Thomas parenting.
(Nancy Thomas, a Colorado layperson trained by Foster Cline to be a “co-therapist” in Rage Reduction, will be keynoting at an adoption training conference in Tennessee Nov 5, 2010, for which social workers can receive continuing education credits. The sponsoring organization of this conference, which receives funding from the Tennessee Department of Children’s Services, advertises that Thomas’ “work was highlighted in an HBO special in 1990 titled, ‘Child of Rage.’”)
In Iowa, Vermont, Colorado, Virginia, New Hampshire, Utah, and Georgia, public funding paid for training therapists in Attachment Therapy. Adoption Subsidy Funding for “special needs children” could pay for any treatment parents wanted, evidence-based or not, including Attachment Therapy.
By 2002, numerous high-profile deaths and child abuse prosecutions resulted in growing professional condemnation of Attachment Therapy. It was at this time that I wrote Schroeder, on behalf of Advocates for Children in Therapy, (ACT) fully expecting she would retract her support.
When Schroeder did not respond, ACT picketed a pricey speaking event in Denver where Schroeder had been chosen to speak because of her “compassion.” Hoping the protest got Schroeder’s attention, I wrote her again:
You obviously did the authors of High Risk (still in print) an enormous favor by writing a foreword, in effect helping to legitimize the message of their book by lending them your well known name and your reputation as a humanitarian. That is viewed by the public as an endorsement of what is said in the book. Do you presently stand by your decision to have written the foreword for the book High Risk?
This time Schroeder responded, albeit briefly:
I am not a doctor and can’t endorse.
When I pressed the issue, she responded:
Writing a foreword and endorsing a medical authority are two different things. I believe books are to stir thoughts, debate, ideas, etc. The more the better. Different theories on everything are detailed in books. That is the best way to vet them.
With such a rationale, it is unclear whether there would be any book Schroeder wouldn’t write a foreword for. Schroeder’s response prompted Wallace Sampson, MD, to comment:
A book is not for discussion or debating. That is what journals are for.
Some years later, when the American Professional Society on the Abuse of Children released its “Task Force Report on Attachment Therapy” (in the journal Child Maltreatment Feb 2006) denouncing Attachment Therapy, its parenting methods and the Attachment Disorder diagnosis, I again wrote Schroeder, hoping that some high level dissing of the practice might make her reconsider her position. She didn’t respond.
Some suggest that Schroeder might not have been aware of High Risk’s contents, and that she is now taking the politically expedient route, hoping the whole issue goes away with time. But while Schroeder has been evasive, she is clearly not regretting her promotion of High Risk. If she was duped, why not jump ship while the jumping is good? While High Risk allowed her to pontificate about her own agenda in the foreword, I have a hard time coming to any other conclusion than that Schroeder may actually approve of this “therapy.” Would someone with presidential aspirations write a foreword for just any book?
At any rate, I think we can assume that Schroeder will not be asking Bantam to remove her foreword from future editions of High Risk, nor will she be calling for legislation that requires federal funding only go to providing evidence-based therapies for adopted children — or any of a dozen other things to help save children from Attachment Therapy.
Schroeder has good reasons to believe her endorsement of Rage Reduction will not tarnish her reputation. She continues to be feted as one of America’s great humanists. Last year, no less than the Center for Inquiry honored her at their 2009 World Congress and highlighted her participation in their Travel Club Adventure Caribbean cruise. CFI officials were not only unconcerned by Schroeder’s association with Attachment Therapy, but accused critics of “nastiness” towards a “defender of good science.”
But it gets worse.
Irony of ironies, Schroeder is now scheduled to keynote for that bastion of evidence-based medicine: The Joint Colloquium of the Cochrane and Campbell Collaborations in Keystone, Colorado, on October 18, 2010.
(As keynoter, Schroeder is billed as the leader of a “multi-year study for the Institute on Civil Society.” But according to ICS, this study produced “no formal document” or publication.)
Last March, I gave a heads up to colloquium organizer Robert Dellavalle, MD, about Schroeder’s unrepentant support of Attachment Therapy. When this yielded no response, I did a broad-spectrum emailing to Cochrane and Campbell officials about this brewing scandal, which prompted Dellavalle to respond:
The leadership discussions so far have noted that invitations to speak at the Colloquium do not constitute an endorsement of any views of the speakers positions past or present. And the topic of your concern is not the topic of Ms. Schroeder’s talk at the meeting.
On learning the title of Schroeder’s keynote is: “Can we keep this Democracy going?” I responded:
We fail to see how this topic is not relevant to the rights of children to be free from actual torture (using the definition of the UN Convention on Torture).
In the same way that world seemed upside down when Bill Maher received the Richard Dawkins Award for scientific integrity, so now do things seem topsy-turvy with CFI and the Cochrane/Campbell Collaborations honoring Schroeder as a defender of science and ethics. This is, alas, not the most shining hour for these otherwise esteemed organizations. Once again, the cult of celebrity scores a bullseye.
See childrenintherapy.org for more information on Attachment Therapy.
See childrenintherapy.org/practitioners for claims made by Attachment Therapy practitioners and proponents.
Linda Rosa, RN, works in home health care in Colorado. She has written about pseudoscientific practices in nursing, such as Therapeutic Touch, and works with Advocates for Children in Therapy to oppose unvalidated and abusive psychotherapy. She currently is Executive Director for the Institute for Science in Medicine.
![]()
Do you have low T?
If you google “low testosterone” you’ll see lots of ads for testosterone replacement. Some are from pharmaceutical companies that sell testosterone, others from obvious snake-oil salesmen.
Both types of ads list vague sets of symptoms, encourage you to believe that they are pathologic, and want to sell you something to make you better. For example, the pharmaceutical company Solvay gives you a handy guide for speaking to your doctor, and a quiz to see if you have “low T”. The quiz asks some questions that may be useful, but also asks very general questions about your sense of well being, and includes this gem:
I don’t feel sick, I just don’t feel like myself anymore. Could I have Low T?
The ad then gives this advice:
Because Low T signs and symptoms may not be clear and apparent, they may seem to be a normal part of aging or assumed to be caused by other health conditions. But talk to your doctor if you have symptoms of Low T. And ask to get tested. All it takes is a simple blood test that can be done during a routine checkup. If you do have Low T, your doctor may recommend treatments that can help bring testosterone up to normal levels and keep them there.
If you have diabetes, you should ask your doctor for a Low T test. The Endocrine Society recommends that all men with type 2 diabetes have their testosterone levels checked. Patients who have been diagnosed with diabetes have an increased chance of also having Low T.
Let’s step back for a moment. What is being claimed is that low testosterone levels in males is a common cause of certain symptoms, and that testosterone replacement therapy can alleviate these symptoms. To evaluate this claim from the perspective of science-based medicine, we need to ask specific questions.
- Is there a plausible connection between testosterone levels and certain symptoms?
- What is a normal testosterone level?
- Are there specific symptoms that correlate with lower levels?
- Does replacement therapy correct these symptoms?
Testosterone is an important hormone in males, and the effects of complete testosterone deprivation are easily observed. Castration has different effects on males depending on whether it is done before puberty or after. Given the effect of total androgen (testosterone) deprivation, it is plausible that partial deficiency may lead to physiologic problems.
Defining normal testosterone levels is problematic though. Most studies show a decline in testosterone levels with age. What is “normal” at 30 is not “normal” at 70. Does this decline correlate with symptoms?

Decline in testosterone level with age
The answer isn’t clear. Studies have shown that low testosterone levels are associated with different symptoms at different ages. In older men with sexual dysfunction, low testosterone levels were associated with severe erectile dysfunction and decreased frequency of intercourse. In younger men, low testosterone levels were associated with a decrease in nocturnal erections and reduced libido. In the middle of the studied age range, there were no significant associations between testosterone levels and sexual symptoms. What this may tell us is that in older men, low levels of testosterone likely contribute to severe symptoms of sexual dysfunction.
The answer to question 2 is that normal testosterone levels vary with age, the type of test used, and the time of day the blood is drawn. Testosterone decreases with age, and this decrease correlates with certain symptoms. Because of these and other data, the recommendation of the Endocrine Society (the most comprehensive and authoritative source) is to restrict the diagnosis of testosterone deficiency to men who have consistent symptoms and an unequivocally low testosterone level.
Question 3 has a difficult answer. As we’ve seen, in certain age groups, certain sexual symptoms correlate well with low T levels. There are some weak associations between less specific symptoms and testosterone deficiency (symptoms such as fatigue, loss of vigor, depressed mood, decreased physical performance). Most of these less specific symptoms can be caused by a variety of problems or by none at all.
So, the data support a connection between certain symptoms and low testosterone levels. Can testosterone replacement therapy (TRT) improve these symptoms?
The evidence is mixed. There seems to be good evidence that testosterone replacement improves libido, but has little effect on erectile dysfunction (especially in younger patients). There is a paucity of placebo-controlled studies of TRT, but non-placebo-controlled trials show some improvements in energy and sense of well-being.
Several medical conditions are correlated with low T. Obesity fairly strongly correlated with low testosterone levels, but there are no consistent data that show an improvement in obesity with TRT.
In sum, testosterone deficiency is a real problem that may affect a small but significant number of men. The symptoms most consistent with low T are sexual problems, especially with age. Replacement therapy seems to help with these symptoms in some men. The ads for testosterone replacement therapy are, in my opinion, very problematic, nearing the point of deception. They seem to link all manner of vague and common symptoms to low T, and imply that the use of their product is likely to fix these problems. These ads explicitly instruct patients to ask for testing that may not actually be required. They shift the focus from a careful, methodical analysis of a difficult problem to frank disease mongering, encouraging the pathologizing of what may be normal symptoms, and offering up a costly therapy that may be no better than placebo, but with additional risk.
References
Corona, G., Mannucci, E., Ricca, V., Lotti, F., Boddi, V., Bandini, E., Balercia, G., Forti, G., & Maggi, M. (2009). The age-related decline of testosterone is associated with different specific symptoms and signs in patients with sexual dysfunction International Journal of Andrology, 32 (6), 720-728 DOI: 10.1111/j.1365-2605.2009.00952.x
Spetz, A., Palmefors, L., Skobe, R., Str??mstedt, M., Fredriksson, M., Theodorsson, E., & Hammar, M. (2007). Testosterone correlated to symptoms of partial androgen deficiency in aging men (PADAM) in an elderly Swedish population Menopause, PAP DOI: 10.1097/gme.0b013e318057786b
Allan, C., Forbes, E., Strauss, B., & McLachlan, R. (2008). Testosterone therapy increases sexual desire in ageing men with low–normal testosterone levels and symptoms of androgen deficiency International Journal of Impotence Research, 20 (4), 396-401 DOI: 10.1038/ijir.2008.22
Reyes-Vallejo, L., Lazarou, S., & Morgentaler, A. (2007). Subjective Sexual Response to Testosterone Replacement Therapy Based on Initial Serum Levels of Total Testosterone The Journal of Sexual Medicine, 4 (6), 1757-1762 DOI: 10.1111/j.1743-6109.2006.00381.x
Bhasin S, Cunningham GR, Hayes FJ, Matsumoto AM, Snyder PJ, Swerdloff RS, Montori VM, & Task Force, Endocrine Society (2010). Testosterone therapy in men with androgen deficiency syndromes: an Endocrine Society clinical practice guideline. The Journal of clinical endocrinology and metabolism, 95 (6), 2536-59 PMID: 20525905
Araujo, A., Esche, G., Kupelian, V., O’Donnell, A., Travison, T., Williams, R., Clark, R., & McKinlay, J. (2007). Prevalence of Symptomatic Androgen Deficiency in Men Journal of Clinical Endocrinology & Metabolism, 92 (11), 4241-4247 DOI: 10.1210/jc.2007-1245
![]()