
 Mass High Tech | Halamka to resign from Harvard Med School CIO post Mass High Tech John Halamka, chief information officer at both Beth Israel Deaconess Medical Center (BIDMC) and Harvard Medical School (HMS), is stepping down from his post at HMS. He announced the news Thursday on his blog, “Life as a Healthcare CIO ... Halamka To Leave Harvard Med School CIO PostInformationWeek |
Monthly Archives: July 2011
UNR closer to buying home in Clark County for medical school dean – Las Vegas Sun
UNR closer to buying home in Clark County for medical school dean Las Vegas Sun Schwenk, who comes to Nevada from the University of Michigan Medical School, started work this month. He has decided to live in Reno, purchasing a home with his money, spokeswoman Anne McMillin said. However, Schwenk would divide his time and attention ... |
Program marks early step toward valley med school – Bakersfield Californian
Merced Sun-Star | Program marks early step toward valley med school Bakersfield Californian Christina Thabit's decision to attend medical school was largely influenced by doctors she met in her Bakersfield hometown, many of whom encouraged her to one day practice in the valley. ... UC Merced sees its first medical studentsABC30.com UC medical students introducedMerced Sun-Star 5 students admitted to UC Merced medical programVisalia Times-Delta KMPH Fox 26 all 9 news articles » |
OSU med school taps Yale prof as dean; Lucey leaving – Bizjournals.com
Columbus Dispatch | OSU med school taps Yale prof as dean; Lucey leaving Bizjournals.com Meanwhile, Dr. Catherine Lucey, who had been interim dean, is leaving Ohio State to become vice dean for education at the medical school of University of California at San Francisco, where she had served her residency in internal medicine. ... Ohio State medical school taps Yale professor as new deanMedCity News OHIO STATE NAMES YALE LEADER AS NEW DEAN OF MEDICINEDOTmed.com |
Galectin Therapeutics Taps Into University of Michigan Expertise – Genetic Engineering News
Genetic Engineering News | Galectin Therapeutics Taps Into University of Michigan Expertise Genetic Engineering News Galectin_Therapeutics entered into a research collaboration with Jose Jalife, MD, of the University of Michigan Medical School, to better understand the relationship of galectin-3 to cardiac fibrosis in chronic cardiac arrhythmias. ... Galectin Therapeutics Announces Research Collaboration with Dr. Jose Jalife of ...MarketWatch (press release) |
Asthma, placebo, and how not to kill your patients
A number of years ago I was walking along Lake Michigan with a friend (a fellow medical resident) when she turned to me and said, “are you wheezing? Do you have asthma?” I had always been physically active and assumed my breathlessness while walking down the trail was due to the thirty extra pounds of pizza and doughnuts I’d acquired during residency. But she was right: I was wheezing and breathless and it didn’t feel good at all. I made an appointment with one of the hospital’s lung docs who took a good history, did a physical, and ran some pulmonary function tests. And I did have asthma. And it felt much, much better when I used proper medication, a feeling confirmed by my improving lung function tests. (Not too surprisingly, the asthma got even better when I lost 40 lbs and started treatment for my acid reflux.)
I still get mild asthma symptoms from time to time, especially when I get sick, but for many others, the picture isn’t so pretty. Asthma kills at least a quarter of a million people every year around the world. If you’ve ever worked in an ER and seen a kid with a bad asthma attack, you’ve earned a healthy respect for the disease. If you’ve ever watched your own kid gasping for breath, begging you to make it better, you’ve learned to fear it.
As our understanding of asthma has improved, so has our ability to treat it (an ability that is strongly linked to a patient’s socio-economic status. Mortality has been rising despite the discovery of better treatments. Wait: let’s pull this out of the parentheses…)… Asthma deaths and hospitalizations are largely preventable, and disproportionately affect Black and Hispanic Americans. We know how to treat the disease asthma, but don’t know how to treat the people who are affected most.
 We understand that asthma is not just a tightening of the airways but also an inflammation that can cause long-term damage. Not only can we treat asthma, but we have objective ways of measuring how well our patients are doing. It’s easy and inexpensive to measure airway obstruction and response to medications. We know what works.
We understand that asthma is not just a tightening of the airways but also an inflammation that can cause long-term damage. Not only can we treat asthma, but we have objective ways of measuring how well our patients are doing. It’s easy and inexpensive to measure airway obstruction and response to medications. We know what works.
For this reason, a new study in the New England Journal of Medicine seems both wise and foolish.
(I thought I was so on the ball. I really did. But while I was busy riding my bike, playing with my kid, and looking at rentals with my wife, David Gorski and my other medical blogger pals were out in Las Vegas at TAM discussing the very study I wanted to tell you about.)
The study, called “Active albuterol or placebo, sham acupuncture, or no intervention in asthma,” was done for reasons that are not clear to me. It may have been done not to test the effectiveness of asthma therapy but to look at what a “placebo” might really be or do. At least, I think that was the idea. When reading the abstract and full text, it’s not actually clear why the study was done. At first it seems as if it were done to see why asthmatics treated with placebo improve:
In prospective experimental studies in patients with asthma, it is difficult to determine whether responses to placebo differ from the natural course of physiological changes that occur without any intervention.
Why ask such a question? We know that poorly-treated asthma is deadly, and well treated asthma much less so. Why do we care about placebo effects here? The authors explain further:
Placebo effects (i.e., benefits resulting from simulated treatment or the experience of receiving care) are reported to improve signs and symptoms of many diseases in clinical trials and in clinical practice. On this basis, the accepted standards for clinical-trial design specify that the effects of active treatment should ideally be compared with the effects of placebo. Despite this common practice, it is unclear whether placebo effects observed in clinical trials (or those that presumably occur in clinical care) influence both objective and subjective outcomes and whether placebo effects differ from the natural course of disease or regression to the mean.
In other words, the authors want to know what placebos actually do to real people, and they chose asthmatics because they are easy to study (there are symptom-assessment tools for subjective data and spirometry for objective data). This makes asthma both the right and wrong choice for the study. It’s an excellent model to assess the affect of placebo, but one in which the use of placebo is hard to justify on an ethical basis.
Not surprisingly, they found that “doing something” worked better than doing nothing. More specifically, they found that any placebo will make a patient feel subjectively better than doing nothing at all. They also found that all three placebos (sham acupuncture, fake inhaled medicine, and simply being enrolled in the study without treatment) improved objective measures of lung function, but not nearly as much as real medicine (in fact, not much at all).
In other words, simply attending to a patient makes them feel better. But to get a significant objective improvement (in asthma at least) you must also give them real medicine. Real medicine comprises both active medications and attending to the patient. There is no separate “placebo” that can be given to treat asthma effectively.
This is actually a quite beautiful study. It demonstrates that “placebo effect” is not the same as a real treatment, that real treatment always includes whatever benefit placebo provides, and that placebo is mostly an effect on subjective rather than objective measures of health. You can’t fix asthma with placebo, only with real treatment. But we’ve already known that from decades of studying asthma. So what other justification is there for doing this study?
Our research has important implications both for the treatment of asthma and for clinical-trial design in general. Many patients with asthma have symptoms that remain uncontrolled, and the discrepancy between objective pulmonary function and patients’ self-reports noted in this study suggests that subjective improvement in asthma should be interpreted with caution and that objective outcomes should be more heavily relied on for optimal asthma care. Indeed, although improvement in objective measures of lung function would be expected to correlate with subjective measures, our study suggests that in clinical trials, reliance solely on subjective outcomes may be inherently unreliable, since they may be significantly influenced by placebo effects. However, even though objective physiological measures (e.g., FEV1) are important, other outcomes such as emergency room visits and quality-of-life metrics may be more clinically relevant to patients and physicians. Although placebos remain an essential component of clinical trials to validate objective findings, assessment of the course of the disease without treatment, if medically appropriate, is essential in the evaluation of patient-reported outcomes. (Emphasis mine, PalMD)
This is folly. First, we have a huge literature on quality of life metrics in asthma. Huge. And we also know that objective changes in asthma are what save patients’ lives. Yes, I care how my patient feels, but it is not more “clinically relevant” than how they are actually doing physiologically. Both are important, but not equal. And the idea that comparing active treatment to placebo is not ideal is not new to researchers. It’s simply that following the natural history of the disease as a “control” is not usually appropriate (cf. Tuskegee syphilis experiment).
No good clinician would consider treating an asthmatic with placebo. Improper treatment of asthma leads to debility and death. This study chose mild asthmatics, but I still feel very uncomfortable with the ethics of the study design. Rather than using a disease we know how to treat to study placebo, we should be finding ways to get treatment to the millions of people who aren’t getting it.
References
Wechsler ME, Kelley JM, Boyd IO, Dutile S, Marigowda G, Kirsch I, Israel E, & Kaptchuk TJ (2011). Active albuterol or placebo, sham acupuncture, or no intervention in asthma. The New England journal of medicine, 365 (2), 119-26 PMID: 21751905
![]()
![]()
![]() <!--<!--
<!--<!--![]()
![]()
![]()
![]()
Dummy Medicines, Dummy Doctors, and a Dummy Degree, Part 1: a Curious Editorial Choice for the New England Journal of Medicine
Background
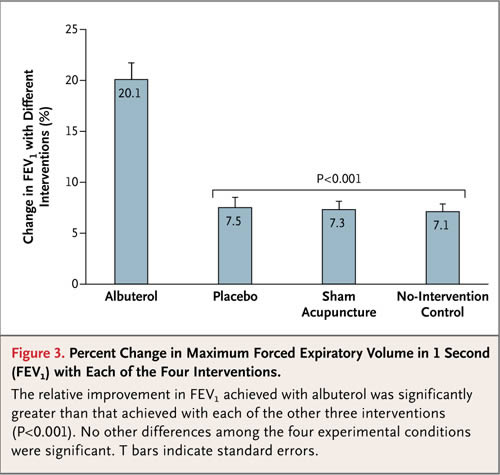
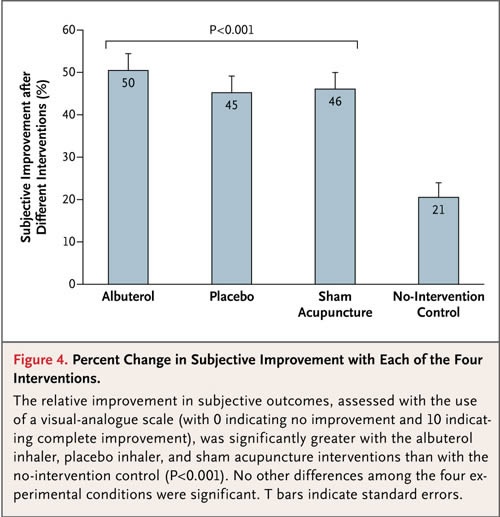
This post concerns the recent article in the New England Journal of Medicine (NEJM) titled “Active Albuterol or Placebo, Sham Acupuncture, or No Intervention in Asthma.” It was ably reviewed by Dr. Gorski on Monday, so I will merely summarize its findings: of the three interventions used—inhaled albuterol (a bronchodilator), a placebo inhaler designed to mimic albuterol, or ‘sham acupuncture’—only albuterol resulted in a clinically important improvement of bronchial airflow; for that outcome the two sham treatments were equivalent to “no intervention.” For all three interventions, however, self-reported improvements were substantial and were much greater than self-reported improvements after “no intervention.” In other words, dummy treatments made the subjects feel better, whereas real medicine not only made them feel better but actually made them better.
Before proceeding, let me offer a couple of caveats. First, the word ”doctors” in the flippant title of this post refers mainly to two individuals: Daniel Moerman, PhD, the anthropologist who wrote the accompanying editorial, and Ted Kaptchuk, the Senior Author of the trial report itself. It does not refer to any of the other authors of the report. Second, I have no quarrel with the trial itself, which was quite good, or with the NEJM having published it, or even with most of the language in the article, save for the “spin” that Dr. Gorski has already discussed.
My quarrels are the same as those expressed by Drs. Gorski and Novella, and by all of us on the Placebo Panel at TAM. This post and the next will develop some of those points by considering the roles and opinions of Moerman and Kaptchuk, respectively.
A True Story
Late one night during the 1960s a friend and I, already in a cannabis-induced fog, wandered into a house that had been rented by one of his friends. There were about 8-10 ‘freaks’ there (the term was laudatory at the time); I didn’t know any of them. The air was thick with smoke of at least two varieties. After an uncertain interval I became aware of a guy who was having trouble breathing. He was sitting bolt upright in a chair, his hands on his knees, his mouth open, making wheezing sounds. He took short noisy breaths in, followed by what seemed to be very long breaths out, as though he was breathing through a straw. You could hear the wheezing in both directions. Others had also noticed that he was in distress; they tried to be helpful (“hey, man, ya want some water or somethin’?”), but he just shook his head. He couldn’t talk. My friend, who had asthma himself, announced that this guy was having an asthma attack and asked if he or anyone else had any asthma medicine. No one did.
No one had a car, either, and for obvious reasons no one, not even the wheezing guy himself, was about to call 911. The nearest hospital was about 5 miles away. My friend said that the thing to do when someone has an asthma attack is leave him alone so he won’t get too excited, and he’ll get through it. Yeah, that must be right, we all figured; he has asthma too so he knows. We were all blowing smoke into the wheezing guy’s face as we expressed our concern.
At some point my friend and I left. The next day I heard that the guy with the asthma attack was eventually taken to the ER after another freak had come along who happened to have a car. The guy did alright, I guess. I don’t really know, but if he’d died I probably would’ve heard about it.
Several years later I went to medical school and began to learn about asthma, and as an internal medicine resident I saw enough patients with acute asthma attacks to realize, in a way that still makes me cringe, just how sick that guy had been and how totally clueless and selfish were we, his supposedly concerned companions. If the freak with the car hadn’t shown up…
Cultural Anthropology and Cultural Relativism
All of which has something to do with the surprise I felt a few days ago upon reading the following in the aforementioned editorial in the NEJM, the world’s most prestigious medical journal:
For subjective and functional conditions — for example, migraine, schizophrenia, back pain, depression, asthma, post-traumatic stress disorder, neurologic disorders such as Parkinson’s disease, inflammatory bowel disease and many other autoimmune disorders, any condition defined by symptoms, and anything idiopathic — a patient-centered approach requires that patient-preferred outcomes trump the judgment of the physician. Under these conditions, inert pills can be as useful as “real” ones…
Let’s see: asthma is a “subjective and functional condition”? In the bad old days of paternalistic medicine, the term “functional” meant “without demonstrable pathology.” It was usually synonymous with ”in your head”—whether the physician openly expressed that opinion or not. Doesn’t sound very “patient-centered” to me. I’m happy to report that you hardly ever hear ”functional” anymore, which reflects at least some measure of social progress for the profession. Since the term’s other possible meanings are nearly limitless and therefore vague beyond utility—every complaint or medical condition is in some way “functional,” after all—it seems reasonable to assume that the editorial’s author intended the old meaning, even if it and “subjective” are redundant.
Yet asthma is based in demonstrable pathology, as are most of the other named conditions, and in most of those (migraines, Parkinson’s disease, inflammatory bowel disease, and “many other autoimmune disorders”) there are specific treatments based on pathophysiology that, like albuterol for asthma, effect substantial, objective and subjective improvements. ”Idiopathic” refers to any condition whose cause is unknown, which includes most of those already mentioned and many other diseases for which medicines are effective for both objective and subjective outcomes (diabetes, Grave’s disease), and even some that are, for practical purposes, curable: Hodgkin’s disease, acute lymphocytic leukemia in children, some testicular cancers (remember Lance?), temporal arteritis, pernicious anemia, and many more. How could the author of a NEJM editorial be unaware of such commonplace medical facts?
The answer is that the author, Daniel Moerman, is not a doctor or even a biomedical scientist. He’s an anthropologist who seems to have confused sentimental and poetic aspects of his major academic interests—native American culture, medicinal plants, and healing rituals—with modern science and medicine. I urge you to consider his CV and the excerpts from his book Medicine, Meaning and the “Placebo Effect,” discussed by Dr. Gorski a few days ago. In the very first chapter he betrays more ignorance of medicine when he expresses surprise that a gastroenterologist didn’t find it odd that in a cohort of experimental subjects given only placebos for peptic ulcer disease, nearly half demonstrated healed ulcers after 4 weeks—about the percentage, I’d wager, whose ulcers would have healed with no trial intervention.
Regarding Prof. Moerman’s view of the sort of science that physicians need to know, along with Dr. Gorski I detect shades of Deepak Chopra, although I also detect a bit of down-home, folksy, isn’t-he-wise midwestern ambiguity, possibly delivered in a Mr. Ed voice, such as to give the good professor a way to deny it all. Consider this excerpt from the NEJM editorial, also noted by Dr. Gorski:
What do we learn from this study? The authors conclude that the patient reports were “unreliable,” since they reported improvement when there was none — that is, the subjective experiences were simply wrong because they ignored the objective facts as measured by FEV1. But is this the right interpretation? It is the subjective symptoms that brought these patients to medical care in the first place. They came because they were wheezing and felt suffocated, not because they had a reduced FEV1. The fact that they felt improved even when their FEV1 had not increased begs the question, What is the more important outcome in medicine: the objective or the subjective, the doctor’s or the patient’s perception? This distinction is important, since it should direct us as to when patient-centered versus doctor-directed care should take place.
Does he really believe that the subjective is the more important outcome? It certainly seems so; next he writes:
In a number of other trials in which both sham and actual treatments were evaluated, results were very similar. In one study of major depressive disorder, placebo, hypericum (St. John’s wort), and sertraline all resulted in about the same level of improvement on the Hamilton Rating Scale for Depression. Similarly, in studies of low back pain in both the United States and Germany, true acupuncture and sham acupuncture had about the same effectiveness yet were substantially better than usual medical care in relieving the pain. A number of surgical procedures — such as arthroscopic knee surgery and spinal vertebroplasty — have led to similar results with actual and sham treatments. In these studies and many more, inert treatments have had effects similar to their “active” analogues.
Woah! Sure, the subjective results of those trials “were very similar” to those of the albuterol trial, but so what? What distinguishes those trials from the albuterol trial is that there were no objective outcomes to measure! Moerman has missed the point of the distinction. He seems to prefer that medicine be about “a profound meaning response,” as he explained in an article written jointly with homeopath Wayne Jonas a few years ago, which comes awfully close to asserting that all “healing” is culturally determined:
Anthropologists understand cultures as complex webs of meaning, rich skeins of connected understandings, metaphors, and signs. Insofar as 1) meaning has biological consequence and 2) meanings vary across cultures, we can anticipate that biology will differ in different places, not because of genetics but because of these entangled ideas…
In the NEJM editorial Prof. Moerman doesn’t seem bothered by an inconvenient truth about objective outcomes. That is, maybe he doesn’t:
Maybe it is sufficient simply to show that a treatment yields significant improvement for the patients, has reasonable cost, and has no negative effects over the short or long term. This is, after all, the first tenet of medicine: “Do no harm.”
Prof. Moerman, what about the harm that comes from the NEJM seeming to judge treatments that offer favorable subjective outcomes as being equivalent to those that offer favorable objective outcomes? This kind of harm, for example. Asthma isn’t just a “subjective and functional condition,” whatever that is. It’s a real and potentially lethal disease. Oh, but you wrote “maybe.” Silly me.
Dr. Drazen, Where art Thou?
It is especially puzzling, considering the identity of its Editor-in-Chief, that the New England Journal of Medicine asked Daniel Moerman to write the editorial to accompany the report of the albuterol study. Jeffrey Drazen is not only a pulmonologist, but an expert in the pathophysiology of asthma. He has been instrumental in developing new drugs for asthma, drugs whose effects—I’m willing to bet, but I’ve no time to research right now—have been demonstrated objectively. If memory serves, Dr. Drazen trained at the old Peter Bent Brigham Hospital under ‘Reggie’ McFadden, whose chapter on asthma in my 2001 edition of Harrison’s Principles of Internal Medicine includes this passage:
The most effective treatment for acute episodes of asthma requires a systematic approach based on the aggressive use of sympathomimetic agents and serial monitoring of key indices of improvement. Reliance on empiricism and subjective assessment is no longer acceptable.
I’d be surprised if Dr. Drazen had ever heard of Moerman before the albuterol report was accepted for publication, and I wonder who recommended him. Kaptchuk, perhaps? Heh.
Unfortunately, someone isn’t minding the NEJM store when it comes to certain dubious topics, as Dr. Gorski mentioned and as I’ve written about previously.
Good News, Bad News
Perhaps Dr. Drazen imagines that the editorial won’t do any real damage, because real doctors will immediately identify it for what it is: Bullshit. That is probably true, except for the small but possibly growing number of “integrative” aficianados out there. I worry more about other Dummy Docs, such as naturopaths (ND=Not a Doctor, according to one apostate), who already believe wholeheartedly what Prof. Moerman “maybe” believes, and a lot more:
For an acute asthma attack try a steam inhalation (draping a towel over your head and a bowl of hot water) with a few drops of eucalyptus oil in the water. Be careful that the water is not so hot that the steam burns your face. Some doctors recommend taking baths with a cup or so of 3% hydrogen peroxide in the water to bring extra oxygen to the entire surface of the skin, thus making the lungs somewhat less oxygen hungry. This method can be performed preventively. Another technique for an acute attack is to drink some hot water with the juice of one clove of garlic. [etc.]
And:
How Can Homeopathy Help Asthma?
Like with Traditional Chinese Medicine, each individual is analyzed for their specific symptoms and an appropriate therapy is chosen, not for the disease, but for the person displaying signs of health out of balance. This is a very important distinction, and, very generally speaking, one of the main differences between conventional and “complementary” approaches to health care.After the homeopath, naturopath or medical doctor trained in homeopathy (they should have the title “Diplomat of Homeopathy” after their other credentials) listen carefully to your story, one of the following remedies are likely to be prescribed. [etc.]
What Kind of Subtle Energy Techniques Are Useful for Asthma?
Some folks like to work with flower essences. Some of the more popular ones to help with asthma are:
- oak
- mimulus
- larch
- wild rose
- hornbeam
- crab apple
- impatiens
- gentian
- Shasta daisy
- blackberry
- chamomile
- agrimony
- clematis
Other people find it useful to work with color, either by using thin plastic filters over light sources in their home or office environment, or by wearing clothes of specific colors. The following serves as a guide to experiment with color therapy to help asthma.
During an asthma attack try:
- purple (raises the threshold of pain and is soporific; is a vasodilator; slows heart rate) on face, throat and chest
- scarlet (acts as a stimulant to the kidney and adrenals) on kidneys
- orange (an antispasmodic) on throat and chest
- indigo or violet on throat, chest and upper back for 15 minutes
Etc., ad nauseam. Boy, do Dummy Docs love it when their pet treatments seem to be endorsed by real medicine, especially the highest bastions of real medicine. Science, even! Is it any surprise when something like this happens? Josephine Briggs, are you reading this? If so, please look here for more discussion of that case. You also won’t want to miss the sequel to this post.
![]()
![]()
![]() <!--<!--
<!--<!--![]()
![]()
![]()
![]()
Salt: More confirmation bias for your preferred narrative
Judging by the recent press reports, the latest Cochrane review reveals that everything we’ve been told about eating salt, and cardiovascular disease, is wrong:
The New York Times: Nostrums: Cutting Salt Has Little Effect on Heart Risk
The Daily Mail: Cutting back on salt ‘does not make you healthier’ (despite nanny state warnings)
Scientific American: It’s Time to End the War on Salt
Sometimes it’s possible to completely miss this point. And that’s what’s happened here.
When it comes to health, it’s the hard outcomes we care about. We pay attention to measures like high blood pressure (hypertension) because of the relationship between hypertension and events like heart attacks and strokes. The higher the blood pressure, the greater the risk of these events. The relationship between the two is well established. So when it comes to preventive health, we want to lower blood pressure to reduce the risk of subsequent effects. Weight loss, diet, and exercise are usually prescribed (though often insufficient) to reduce blood pressure. For many, drug treatment is still required.
There is reasonable population-level data linking higher levels of salt consumption with higher blood pressure. From a population perspective, interventions that dramatically lower salt intake result in lower blood pressure. Not everyone responds in the same way — many people with normal blood pressure can regularly consume a high salt load without any apparent change in blood pressure. But not everyone, and not forever. Salt sensitivity seems to increase with age and is more pronounced in some ethnic groups, as well as in those with salt-sensitive conditions such as kidney disease. And chronic high levels of salt consumption may be associated with the subsequent emergence of hypertension. There may be additional effects, unrelated to blood pressure, too. However, the causality between salt consumption, and all of these negative effects, is less clear.
So does reducing dietary salt reduce cardiovascular events? That’s the key question. To definitively answer the question, we’d randomize patients to high- and low-sodium diets, force them to follow these diets for years or decades, and monitor consumption, blood pressure, and cardiovascular events. We’d also want to explore the factors that seem to make some more sensitive to the effects of salt than others. To ensure we could see a difference (if it exists), we’d need a large sample size — hundreds or thousands of people, ideally. See any problems with the feasibility? Like any dietary intervention trial, this type of study would be exceptionally difficult to do — forcing dietary changes is very difficult, and cannot be done in a blinded manner. Even randomization is unlikely to be effective in ensuring there’s adherence — established dietary habits don’t lend themselves to long-term change easily. So we must look to lower-quality evidence — inferences from observational studies that have tracked consumption, or indicators like blood pressure and salt consumption in the short-term. And there are fair criticisms of the data. Some see relationships, and others dismiss them.
When it comes to clinical practice guidelines, low salt diets are the mainstays of pretty much every set of guidelines on the management of high blood pressure. The evidence supporting the relationship with hard outcomes is robust, but not rock-solid. We don’t have causal data, but we do have considerable epidemiologic evidence to suggest that reducing dietary salt consumption is likely to offer net benefits in the management of hypertension.
And that’s where the recommendations to cut salt come from. The vast majority of the salt we eat (75%) is from processed foods. Restaurants are a large source, too. Few foods in their original state are naturally high in salt, and in general, we don’t add that much at the table. Interestingly, when foods are reduced in sodium, we don’t tend to add the same amount back at the table. So public health initiatives have concentrated on a few strategies: education on how to reduce your own salt consumption, and putting pressure on packaged food manufacturers to reduce the amount of sodium that they use in their products. But reducing salt may hurt sales: if we’re accustomed to eating salty foods, low-salt foods taste unpalatable. Just last week Campbell Soup Company announced that it’s raising the salt content in its products in an attempt to boost sagging sales.
So do dietary intervention strategies work? That’s what a recent Cochrane review attempted to answer. But you wouldn’t know it, based on the headlines above. Scientific American described the paper as:
This week a meta-analysis of seven studies involving a total of 6,250 subjects in the American Journal of Hypertension found no strong evidence that cutting salt intake reduces the risk for heart attacks, strokes or death in people with normal or high blood pressure.
Eating less salt will not prevent heart attacks, strokes or early death, according to a major study.
Its findings contradict all recommendations by the Government and medical profession urging the public to reduce the amount of salt they consume.
Neither statement accurately describe the findings. Rod Taylor and colleagues set out to do a meta-analysis of dietary intervention studies. They analyzed only studies that measured the effects of dietary interventions that restricted salt consumption, or where the intervention was advice to reduce salt consumption. This was an update of a prior analysis.
Seven studies made up this meta-analysis, including 6,489 patients in total. Three studies looked at those with normal blood pressure, two included patients with high blood pressure, and one was a mixed population, including patients with heart failure. The overall effect? Interventions had small effects on sodium consumption, which led to small effects on blood pressure. There was insufficient information to analyze the effects on cardiovascular disease endpoints.
The authors go on to make the following point, which was ignored in the media coverage:
Our findings are consistent with the belief that salt reduction is beneficial in normotensive and hypertensive people. However, the methods of achieving salt reduction in the trials included in our review, and other systematic reviews, were relatively modest in their impact on sodium excretion and on blood pressure levels, generally required considerable efforts to implement and would not be expected to have major impacts on the burden of CVD.
The authors did not conclude that reducing salt consumption is ineffective. They concluded that interventions such as dietary advice, do not result in substantial reductions in consumption. As expected, blood pressure didn’t change much as a consequence. This finding should not be a surprise. Given the vast majority of salt is consumed via processed foods, it should come as no surprise that dietary approaches are modestly effective at reducing consumption.
Despite the modest and equivocal results, the authors seem to have lost the narrative on their own research findings:
Professor Rod Taylor, the lead researcher of the review, is ‘completely dismayed’ at the headlines that distort the message of his research published today. Having spoken to BBC Scotland, and to CASH, he clarified that the review looked at studies where people were advised to reduce salt intake compared to those who were not and found no differences, this is not because reduced salt doesn’t have an effect but because it’s hard to reduce salt intake for a long time. He stated that people should continue to strive to reduce their salt intake to reduce their blood pressure, but that dietary advice alone is not enough, calling for further government and industry action.
Conclusion
The true finding from the Cochrane review is that dietary interventions to reduce salt intake are largely ineffective at reducing salt consumption. Salt’s impact on cardiovascular events is less clear than its effects on blood pressure. And the long-term benefits of population-level interventions to reduce dietary salt consumption are not yet well established. Until the data are more clear, you can find the data to support whatever narrative you believe. If you want to demonize salt and ignore other factors that contribute to poor cardiovascular outcomes, you can do that. And if you believe that interventions to reduce salt consumption are misguided and unwarranted, and symptomatic of an overreaching nanny state, then you can find data to support that position, too.
My personal take is that most of us will ultimately end up with salt-sensitive conditions. Odds are good we’ll be hypertensive, too. Gradually reducing our chronic salt consumption would seem to be a conservative approach — not by focusing strictly on the salt, but by working to reduce the consumption of salty, processed foods, and substituting healthier, more nutritious choices instead. But I won’t worry when I finish an entire bag of chips — I’ll consider it in the context of an overall strategy: a diet that minimizes processed foods, maintaining an appropriate weight, and getting regular physical exercise.
Reference
Taylor RS, Ashton KE, Moxham T, Hooper L, & Ebrahim S (2011). Reduced dietary salt for the prevention of cardiovascular disease. Cochrane database of systematic reviews (Online), 7 PMID: 21735439
![]()
![]()
![]() <!--<!--
<!--<!--![]()
![]()
![]()
![]()
Behavior and Public Health – To Nudge or Legislate
As health care costs rise and great attention is being paid to the health care system in many countries (perhaps especially the US), the debate is heating up over how to improve public health. Many health problems are greatly increased by the lifestyle choices individuals make – smoking, weight control, and exercise to name a few. The problem is that it is notoriously difficult to change behavior.
There are different ways to approach the challenge of improving lifestyle choices to reduce chronic illness. We can take actions aimed at the individual or aimed at society. These actions can gentle or passive (the so-called “nudge theory”), or they can be more draconian, such as banning certain activity. We can, of course, do all of these things simultaneously, and may need to in order to have a significant impact.
Affecting Individual Behavior
A common criticism of mainstream physicians is that they do not have much impact on the lifestyle of their patients. This is largely true – although there is no convincing evidence that any practitioners have a significant impact on lifestyle. This is mainly the result of the fact that it is extremely difficult to get people to change their behavior.
The default tactic has been to give people information on the assumption that they will then be able to make a rational choice about their health. Psychologists have long known that we are much more likely to simply rationalize our behavior than take the more difficult path of changing it. This is true even of the “scared straight” approach – trying to frighten people with scary images or stories about lung cancer or diabetes.
It is true that physicians can affect patient behavior. For example, even brief physician counseling to quit smoking (less than 5 minutes) increases smoking cessation by 1.6 times. This sounds impressive, but this only increases the rate to 2-10%. Even if we use the higher number in that range, a 10% decrease in unhealthy behavior is very modest (worthwhile, but still modest). It seems that in general you can get about 5% of people to change their behavior with counseling alone. Meanwhile, using medications to aid smoking cessation (nicotine patches and bupropion) can result in up to a 35% decrease in smoking.
The technology of changing individual behavior is advancing, however. The strategy of giving information and assuming rational behavior, while still useful, is highly limited and not sufficient. Psychologists recognize that the way to alter behavior is through psychosocial interventions – exploiting human psychology and peer pressure. One such technique is called motivational interviewing. Essentially, the patient is asked leading questions that gets them to to state their own health goals and concerns. Apparently we are better at persuading ourselves than being persuaded by others.
Sounds good, and generally the research shows that this approach is an improvement – but the effect size is still depressingly small. A systematic review of motivational interviewing for smoking cessation, for example, revealed only a 1.27 relative increase in cessation. So spending 5 minutes with a patient once improves smoking cessation by 1.6 times, and spending multiple 20 minutes sessions of motivational interviewing increases success a further 1.27 times. This is worthwhile in terms of public health outcomes, but it does look like such methods yield diminishing returns.
Motivational interviewing may be more effective for behaviors not related to addiction, such as weight loss and exercise. But still there is huge room for improvement.
Public Health Measures
It is increasingly looking like the way to have a huge impact on public health is at the societal, not individual, level. The goal is to make healthful lifestyle choices easier. Using heavy-handed legislation, however, is not popular (at least not in the US). Such strategies evoke images of a Big Brother nanny state trying to take away our freedoms. There are legitimate concerns about draconian state measures, especially if they are not rigorously science-based, but the looming health care crisis is making public health measures seem more attractive.
One approach is simply to ban unhealthy behavior. Outright bans of products, such as alcohol, have a disastrous history. Another alternative is to restrict the use of such products in certain locations and situations. The best example of this strategy is banning smoking in public locations. A systematic review of 10 studies indicates that such bans reduce the incidence of myocardial infarction in the population by an average of 17%. Banning smoking in public seems to be a clear public health win.
But banning unhealthy behavior gets more tricky when not dealing with addictive substances. Bans of fatty or high-calorie food, for example, are likely to meet much more resistance than restrictions on public smoking. New York City’s ban on trans fat, for example, has been highly controversial. Other states are considering laws to ban toys in kid’s meals, limit advertising, and limiting marketing behavior such as inviting fast food patrons to “go large.”
Resistance to heavy handed strategies has led to the proposal of the nudge theory – using more subtle legislation to influence behavior. Nudge strategies include printing the calories next to menu items. This is a situation in which information is likely to have a significant impact on behavior – because it addresses what may be a significant contributor to the increase in obesity. It is easy to consume far more calories than we think, especially when restaurants prepare menu items that are calorie dense in order to make them tasty and appealing. Having calorie information right in front of you when making menu choices does reduce caloric intake (in this study by 250 calories), although again, not as much as we might hope.
Another nudge approach is to make healthful choices the default choice. This still leaves consumers the freedom to choose what they want, but many more people will go with the healthier choice if it is the default.
Yet another approach is to regulate manufacturers. At present voluntary guidelines are being suggested, and the debate is ongoing about using legislation to require food manufacturers, for example, to produce healthier and lower calorie products. The public has been passively eating more calories simply because the products they buy contain more calories. They have also been lulled by false security – low fat products tend to make up their calories in carbohydrates, while low-carb products make up their calories with increased fat. Either way people eat more because they feel they are eating a healthier products.
Conclusion
It is clear that we need to take a long science-based look at public health and ways to improve lifestyle choices. We need to reverse the obesity epidemic and further reduce smoking. Doing so is not easy – there is no silver bullet to changing human behavior. It is likely that we will need to use a combination of strategies while researching new and better ways to influence behavior.
![]()
![]()
![]() <!--<!--
<!--<!--![]()
![]()
![]()
![]()
Antidepressants and Effect Size
Antidepressant drugs have been getting a bad rap in the media. I’ll just give 3 examples:
- On the Today show, prominent medical expert
 Tom Cruise told us Brooke Shields shouldn’t have taken these drugs for her postpartum depression.
Tom Cruise told us Brooke Shields shouldn’t have taken these drugs for her postpartum depression. - In Natural News, “Health Ranger” Mike Adams accused pharmaceutical companies and the FDA of covering up negative information about antidepressants, saying it would be considered criminal activity in any other industry.
- And an article in Newsweek said “Studies suggest that the popular drugs are no more effective than a placebo. In fact, they may be worse.”
Yet psychiatrists are convinced that antidepressants work and are still routinely prescribing them for their patients. Is it all a Big Pharma plot? Who ya gonna believe? Inquiring minds want to know:
- Are antidepressants more effective than placebo?
- Has the efficacy of antidepressants been exaggerated?
- Is psychotherapy a better treatment choice?
The science-based answers to the first two questions are clearly “Yes.” The best answer to the third question is “It depends.”
In 2008, Erick Turner and four colleagues published an article in The New England Journal of Medicine (NEJM) entitled “Selective Publication of Antidepressant Trials and Its Influence on Apparent Efficacy.” The FDA is able to make sure that drug companies don’t pick and choose which trials, and which outcomes within those trials, get seen. Using clinical trial data from the FDA as a gold standard, Turner, et. al. examined how these same trials were reported in published journal articles, They found that:
…according to the published literature, the results of nearly all of the trials of antidepressants were positive. In contrast, FDA analysis of the trial data showed that roughly half of the trials had positive results.
And some of the negative trials were published with a “spin” that made them appear positive. The data did show that each drug was superior to placebo, but the true magnitude of that superiority was less than a diligent literature review would indicate. They warned that
By altering the apparent risk–benefit ratio of drugs, selective publication can lead doctors to make inappropriate prescribing decisions that may not be in the best interest of their patients and, thus, the public health.
Irving Kirsch has been outspoken about antidepressants’ alleged lack of efficacy. In a controversial meta-analysis published in 1998, he found that placebos provided approximately 75% of the improvement provided by active drug. He suggested that the other 25% is debatable and could be due to an enhanced placebo response when patients experience side effects that convince them they are getting an active drug. In a further study in 2002, he “questioned the clinical significance of antidepressants.”
Kirsch recently looked at the FDA data for 4 of the 12 drugs that Turner examined. In spite of the smaller sample, where Turner found an effect size of 0.31, Kirsch got 0.32. So they got almost exactly the same result. But it was their interpretations of that result that were very different. Kirsch concluded that antidepressants are ineffective, while Turner found that the drugs were indeed superior to placebo. As the figure below shows, each drug’s effect size was positive. Also, none of the confidence intervals overlapped zero. This means that, while there is some probability that the true effect size is zero, meaning that antidepressants and placebo are equal in efficacy, that probability is negligibly small.

The discrepancy between Turner’s and Kirsch’s interpretations hinges on what these effect size numbers mean in terms of clinical significance,. Values of 0.2, 0.5, and 0.8 were once proposed as small, medium, and large effect sizes, respectively. The psychologist who proposed these landmarks admitted that he had picked them arbitrarily and that they had “no more reliable a basis than my own intuition.” Later, without providing any justification, the UK’s National Institute for Health and Clinical Excellence (NICE) decided to turn the 0.5 landmark (why not the 0.2 or the 0.8 value?) into a one-size-fits-all cut-off for clinical significance. In an editorial published in the British Medical Journal (BMJ), Turner explains with an elegant metaphor: journal articles had sold us a glass of juice advertised to contain 0.41 liters (0.41 being the effect size Turner, et al. derived from the journal articles); but the truth was that the “glass” of efficacy contained only 0.31 liters. Because these amounts were lower than the (arbitrary) 0.5 liter cut-off, NICE standards (and Kirsch) consider the glass to be empty. Turner correctly concludes that the glass is far from full, but it is also far from empty. He also points out that patients’ responses are not all-or-none and that partial responses can be meaningful.
Incidentally, NICE is no longer using the 0.5 effect size cutoff.
If we followed Kirsch’s interpretation and rejected antidepressants, how would we treat depression? Psychotherapy avoids the side effects of drugs, but it has its own drawbacks: it is expensive, time-consuming, and variable in quality. How effective is psychotherapy? Psychotherapy trials also suffer from publication bias, just like antidepressant drugs. And when one weeds out low quality studies, psychotherapy has an effect size of only 0.22, lower than the value for antidepressants reported by Kirsch himself, So if we reject any treatment below the (arbitrary) 0.5 cutoff, when a mental health care provider is faced with a patient in need of help, is he or she to do nothing at all?
I don’t doubt that antidepressants have sometimes been over-prescribed and used inappropriately for lesser levels of depression where they are less effective or even ineffective, but this is probably true for psychotherapy, as well. On the other hand, it has been estimated that only about half of depressed patients are getting any kind of treatment. Severe depression is a life-threatening disease. A recent study showed that antidepressants reduced the risk of suicide by 20% in the long term. The risk/benefit ratios are still not clear cut for either form of treatment.
Once more, science fails to give us the black-and-white answers we crave. And once again we are reminded that we can’t rely on the media for accurate, nuanced information about medical science.
For his assistance in preparing this article and for providing the figure, I want to thank Erick Turner, M.D., Department of Psychiatry, Oregon Health and Science University; Staff Psychiatrist, Portland Veterans Affairs Medical Center; Former reviewer, FDA.
![]()
![]()
![]() <!--<!--
<!--<!--![]()
![]()
![]()
![]()
Spin City: Using placebos to evaluate objective and subjective responses in asthma
As I type this, I’m on an airplane flying home from The Amazing Meeting 9 in Las Vegas. Sadly, I couldn’t stay for Sunday; my day job calls as I’ll be hosting a visiting professor. However, I can say—and with considerable justification, I believe—that out little portion of TAM mirrored the bigger picture in that it was a big success. Attendance at both our workshop on Thursday and our panel discussion on placebos on Saturday was fantastic, beyond our most optimistic expectations. There was also a bit of truly amazing serendipity that helped make our panel discussion on placebo medicine an even bigger success.
If there’s one thing about going away to a meeting, be it TAM or a professional meeting, it’s that it suddenly becomes very difficult for me to keep track of all the medical and blog stuff that I normally keep track of and nearly impossible to keep up with the medical literature. This is the likely explanation for why I had been unaware of a study published in the New England Journal of Medicine (NEJM) on Thursday that was so relevant to our discussion and illustrated out points so perfectly that it was hard to believe that some divine force didn’t give it to us in order to make our panel a total success.
Just kidding. It was TAM, after all. It was, however, embarrassing that I didn’t see the study until the morning of our panel, when Kimball Atwood showed it to me.
Before I get to the meat of this study and why it fit into our nefarious plans for world domination, (or at least the domination of medicine by science-based treatments), a brief recap of the panel discussion would seem to be in order. First, for the most part, we all more or less agreed that the term “placebo effect” is a misnomer and somewhat deceptive because it implies that there is a true physiologic effect caused by an inert intervention. “Placebo response” or “placebo responses” seemed to us a better term because what we are observing with a placebo is in reality a patient’s subjective response to thinking that he is having something active done having something done. In general, we do not see placebo responses resulting improvement in objective outcomes; i.e., prolonged survival in cancer. The relative contributions of components of this response, be they expectancy effects (if you expect to feel better you likely will feel better), conditioning, or one that is frequently dismissed or downplayed, namely artifacts of the design of randomized clinical trials and even subtle (or even not-so-subtle) biases in trial design. This issue of placebo responses being observed only in subjective patient-reported clinical outcomes (pain, anxiety, and the like) and not in objectively measured outcomes is an important one, and it is one that goes to the heart of the NEJM study that so serendipitously manifested itself to us. As Mark Crislip so humorously pointed out, the placebo response is the beer goggles of medicine (this is not a spoiler or stealing Mark’s line; several TAM attendees have already tweeted Mark’s line), and much of what is being observed are changes in the patient’s perception of his symptoms rather than true changes in the underlying pathophysiology. This study drove the point home better than we could.
Another point discussed by the panel is also quite relevant. As more and more studies demonstrate very convincingly that “complementary and alternative medicine” (CAM) or “integrative medicine” (IM) therapies do not produce improvements in symptoms greater than placebo. Moreover, multiple studies, including a famous NEJM meta-analysis and a recently updated Cochrane review, demonstrate, placebo responses probably do not constitute meaningful responses. In light of these findings, CAM apologists, driven by ideology rather than science and masters of spin, have begun to admit grudgingly that, yes, in essence their treatments are elaborate placebos. Not to be deterred, instead of simply concluding that their CAM interventions do not work, they’ve moved the goal posts and started to try to argue that it doesn’t matter that CAM effects are placebo effects because placebos are “powerful” and good and—oh, yes, by the way—there are a lot of treatments in science-based medicine that do little better than placebos. In other words, CAM advocates elevate the subjective above the objective and sell the subjective, and that’s exactly what they are doing with this study.
Perception versus physiology
The study under question was performed at Harvard, with Michael E. Wechsler as its first author and Ted Kaptchuk as its senior author. Studies done by groups including Ted Kaptchuk have actually presented us here at SBM with copious blog fodder before, all designed to promote placebo medicine, either through making an argumentum ad populum, claiming in a truly Humpty Dumpty moment that it is possible to have placebo effects without deceiving the patient, and or rebranding of exercise as “alternative” in the New England Journal of Medicine (NEJM) last year.
The current study is entitled, Active Albuterol or Placebo, Sham Acupuncture, or No Intervention in Asthma. Personally, I like this title. It’s a fine title, as it tells the reader in essence what the trial design is in only a few words. And it’s actually a reasonably good pilot study. Of course, it’s not so much the trial design that goes disastrously awry. Rather, it’s the interpretation of the results of the RCT that devolves into propaganda for quackademic medicine in which subjective improvement is used to argue that placebo medicine is good, even when no objective improvement is observed in a disease for which we have good drugs that produce objective improvements as well as subjective improvements.
This study basically compared four different interventions
- Treatment with Albuterol
- Sham acupuncture using the classic retractable needle (note that this was only single-blinded)
- Placebo inhaler
- No treatment at all
Inclusion criteria were as follows:
- Men and women age>or= 18 with a diagnosis of asthma
- Meet American Thoracic Society diagnostic criteria for asthma
- Currently using a stable asthma regimen (no med. changes for 4 weeks)
- Ability to withhold short-acting bronchodilators for 6 hours prior to each visit (see Spirometry description)
- Ability to withhold long-acting bronchodilators for 48 hours prior to each visit (see Spirometry description)
- Presence of reversible airflow obstruction as demonstrated by an improvement in FEV1 of at least 12 % following the inhalation of a ?-agonist after 10 am. at screening visit.
Exclusion criteria were straightforward:
- Lung disease other than asthma
- Respiratory tract infection within the last month
- Active tobacco use
- Asthma exacerbation requiring the use of systemic
- corticosteroids within the past 6 weeks
- Prior experience with acupuncture
These criterial guaranteed that the patients selected have only mild to moderate asthma with no complications from the asthma, such as pneumonia or pulmonary fibrosis. Of course, it would be highly unethical to take people with severe asthma off of their bronchodilators; so medical ethics pretty much prevents testing placebos on people with more severe disease. Still, I can’t help but wonder whether the results reported would have been different in more severe asthma and if the subjective improvement would have been nearly as great. In any case, this study ended up including 39 patients, after 79 were screened, 46 underwent randomization, and 7 dropped out during the protocol. Patients who completed the protocol underwent the following procedure:
These patients returned within a week and were assigned to a randomly ordered series of four interventions — active albuterol inhaler, placebo inhaler, sham acupuncture, or no-intervention control — administered on four separate occasions, 3 to 7 days apart (block 1) (Figure 2). This procedure was repeated in two more blocks of four visits each (blocks 2 and 3), during which the interventions were again randomly ordered and administered. Thus, each subject received a total of 12 interventions. Albuterol and the placebo inhaler were administered in a double-blind fashion and sham acupuncture in a single-blind fashion, and the no-intervention control was not blinded. As before, short-acting and long-acting bronchodilator therapy was withheld for 8 hours and 24 hours, respectively, before each intervention. The no-intervention control condition differs from the natural history of asthma, since it controls for nonspecific factors such as attention from study staff, responses to repeated spirometry, regression to the mean, natural physiological variation, and any effects arising from the hospital setting. Nonetheless, no-intervention controls are the best approximation of no treatment in an experimental design. The study was conducted in accordance with the protocol (available at NEJM.org).
I’m not entirely sure why Kaptchuk thought he had to place a comment in there about no-intervention controls being only an approximation of no treatment in an experimental design. After all, that’s the sort of thing that clinicians and clinical researchers simply know; it does not need to be pointed out to them, much as it shouldn’t need to be pointed out that an RCT is an intentionally artificial method designed to remove as many biases as possible. Be that as it may, one thing that is clear is that these patients could not have truly severe asthma. Ruling out anyone requiring steroids for an acute exacerbation in the recent past and only including patients who could be off their long-acting bronchodilators for 48 hours and their short-acting bronchodilators for 6 hours pretty much guaranteed that.
Everyone’s heard the old cliche that a picture is worth a thousand words, and this is exactly the sort of situation where that’s true. All I need to do is to show you two graphs, and instead of one of my usual 5,000 word blog posts, you can have a 4,000 word post. Funny how that works. In any case, for your edification, here a graph of the objective results of this study, namely the FEV1 for the four groups:
(Click to embiggen)
Not surprisingly, a known, effective bronchodilator had a very strong effect on the actual, objectively measured lung function of these patients. However, it should be noted that all groups improved, even the no-treatment group; it just improved much less than the albuterol group, and the sham acupuncture and placebo albuterol groups were indistinguishable from the no-treatment arm. In fact, in the supplemental data, there is also a table showing that in 32 of the patients exhaled nitric oxide (FENO) was measured, with identical results. Immediately after treatment, FENO increased in patients treated with double-blind albuterol by 5.9%, in contrast to patients treated with placebo inhaler, placebo acupuncture, and no treatment, all of whom demonstrated no significant change in FENO. This graph is about as clear and compelling evidence as there can be within the limits of a relatively small trial, that placebo responses do not change the underlying physiology of the disease of asthma or produce any objectively measurable improvements in lung function the way that real medicine does.
Now, for your edification and comparison, here is a graph of the self-reported subjective improvements.
(Click to embiggen.)
The results are pretty striking, aren’t they? They were so striking that Steve couldn’t resist flipping back and forth between these two graphs for several seconds in order to drive home the point to the audience. The albuterol, sham acupuncture, and placebo albuterol groups all demonstrated a significant improvement in symptoms, while the no-intervention control did not. However, here’s an important point. The scale used was a visual analog scale from 0 to 10 in which 0 means no improvement and 10 means complete resolution. So, again, even though the albuterol, sham acupuncture, and placebo albuterol groups all demonstrated subjective improvement, so did the no-treatment control arm, just less. In other words, all groups reported improvement, even those who received no treatment.
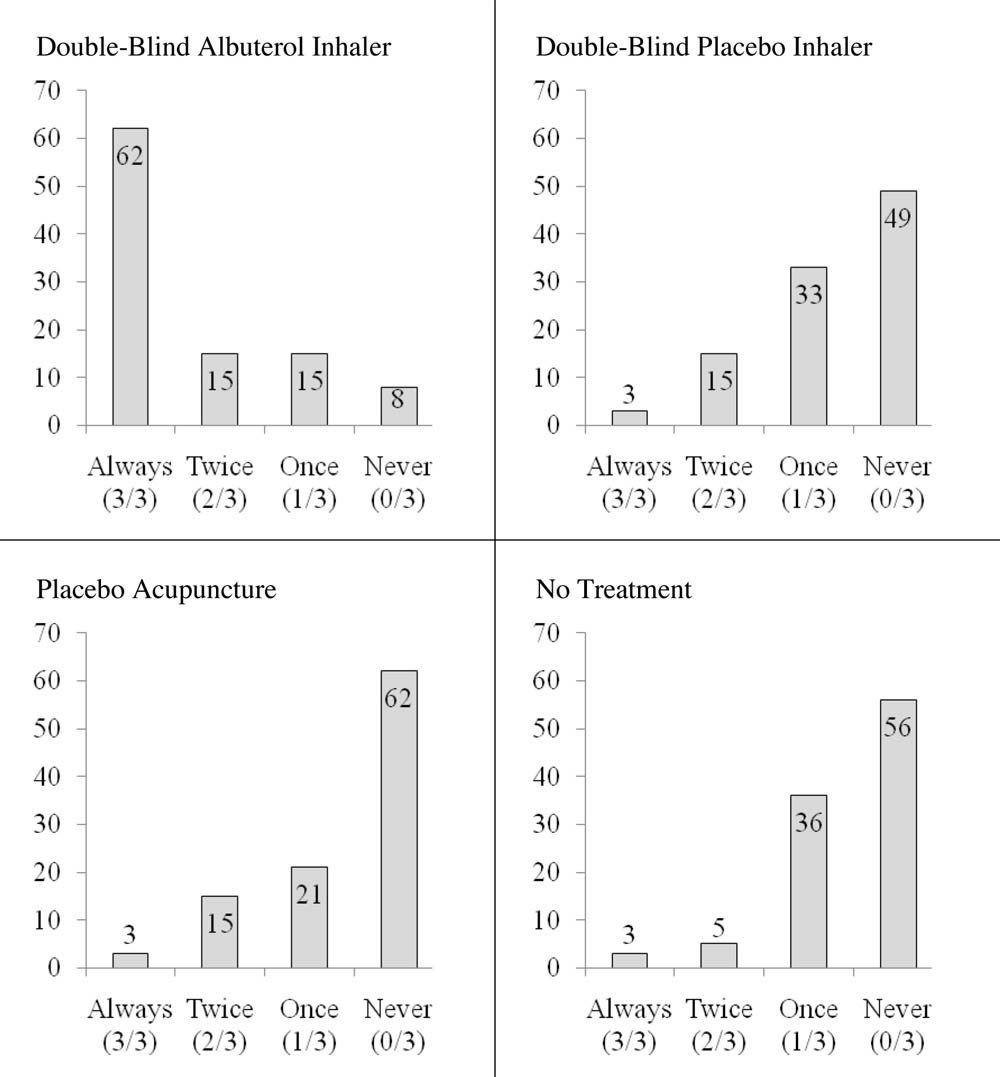
There’s another graph buried in the back of the supplemental data that I now wish we had also shown. Basically, it’s a look at how many patients responded objectively to treatment, as defined by an improvement in FEV1 of 12% or more, at each of the three sessions they did. The results and pattern are striking
(Click to embiggen.)
Notice that, as expected, the vast majority of the patients responded at each session to the albuterol (3/3 sessions). In contrast, only 3% of patients responded 3/3 times to placebo, sham acupuncture, or no treatment. In fact, what’s striking is how similar the three graphs look and how different they look from the graph of patient responses to albuterol. Again, the message is very clear: Real medicine produces real, objectively measurable changes in physiology towards a more normally functioning state. Placebo medicine does not. In any rational, science-based discussion, this would be the end of the story. Placebos don’t work in asthma.
But that’s not the message that was being spread about this story, and here’s where the NEJM, less than a year after its massive fail in publishing a credulous Michael Berman acupuncture article and a clever bait-and-switch article looking at Tai Chi in fibromyalgia, allowed quackademic language to try to make left right, up down, and a negative result an indication that placebo medicine is a good thing.
Spin, spin, spin, spin
As I read the discussion of this paper, I could almost hear the cracking of bones as Kaptchuk went into major contortions to try to explain his negative result. Even though nowhere did the authors really explicitly state their real hypothesis, the design of the study made it painfully clear to anyone who understands clinical research that their hypothesis going in was that placebo responses would result in changes in objectively measured lung function in asthma. They were sorely disappointed, and the contortions of language that went into the discussion were plain to see. The authors implied that it might have been their use of a new, not really validated, patient-reported measure of asthma improvement. Or maybe, they argue, FEV1 isn’t a good measure of the severity of constriction of the airways in asthma, even though spirometry has been a reliable, well-validated test for asthma severity for decades. This is especially true in an academic medical center with a lot of pulmonary specialists. While spirometry can be unreliable in primary care settings and other settings where there isn’t a lot of experience performing it, such a description does not apply to Harvard-affiliated hospitals. At least I would hope not.
Overall, the spin on this study is not that placeboes don’t result in objectively measurable improvements, which is the correct conclusion. Rather, the spin is that subjective symptoms are as important or more important than objective measures; so let’s use placeboes. In the paper itself, Kaptchuk doesn’t quite say that. He first makes a perfectly reasonable point that, if subjective and objective findings don’t correlate, go with the objective findings. Then he does some handwaving:
Indeed, although improvement in objective measures of lung function would be expected to correlate with subjective measures, our study suggests that in clinical trials, reliance solely on subjective outcomes may be inherently unreliable, since they may be significantly influenced by placebo effects. However, even though objective physiological measures (e.g., FEV1) are important, other outcomes such as emergency room visits and quality-of-life metrics may be more clinically relevant to patients and physicians.
My jaw dropped when I read this. “Other outcomes” besides objective measures of disease severity may be “more clinically relevant”? The spin goes way beyond that, though. I have to think that the reviewers kept the authors from getting too frisky with their desire to advocate placebo medicine and promote subjective outcomes as being more important than objective outcomes. No such restraint seemed to inhibit the author of the accompanying editorial, Daniel E. Moerman, Ph.D., who, alas, appears to be based practically in my back yard at the University of Michigan-Dearborn. I had never heard of him before; so I did what all bloggers do when they encounter an unknown. I Googled him. His CV is here, and this is what I found:
Daniel E. Moerman is the William E. Stirton Professor of Anthropology at the University of Michigan — Dearborn, so recognized for his distinguished scholarship, teaching, and professional accomplishments. Because of his work in the field of Native American ethnobotany, Professor Moerman often receives calls from the American Indian community, such as an inquiry from the Menominee in Wisconsin, asking him what kinds of plants they should include in the restoration of their indigenous ecosystem. He acknowledges that we are deeply indebted “to those predecessors of ours on the North American continent who, through glacial cold in a world populated by mammoths and saber-toothed tigers, seriously, deliberately, and thoughtfully studied the flora of a new world, learned its secrets, and encouraged the next generations to study closer and to learn more. Their diligence and energy, their insight and creativity, these are the marks of true scientists, dedicated to gaining meaningful and useful knowledge from a complex and confusing world.”
He’s also known for having written a book entitled Medicine, Meaning and the “Placebo Effect,” part of which can be found here, in particular this doozy of a quote:
There is much objection among physicians to the very existence of something called the placebo effect. It often seems to bother doctors enormously that the fact of receiving medical treatment (rather than the content of medical treatment) can initiate a healing process. Why? I think it is because medicine is rich in a particular kind of science. Medical education is filled with science. In the US, all students must score high on the “Medical College Admission Test” in order to be admitted to medical school. Students are allowed a total of 345 minutes to complete the exam. Eight five minutes are devoted to “verbal reasoning,” and 60 minutes to “writing sample.” The remaining 200 minutes (58.5%) are split evenly between “physical sciences” and “biological sciences.” It is apparently important that physicians understand levers, inclined planes, the acceleration of falling bodies, the life cycle of insects, and the process of photosynthesis. The kind of science that doctors have to learn is the simpler sort of science, the mechanical kind. Physicists worked out the mechanics of simple machines (levers, planes) in the seventeenth century. In our times, they have been working on much slipperier subjects: quarks, chaos, the “weak force,” and the oddest of quantum phenomena. Cause and effect are far less easy to detect in these matters than in the study of falling bodies…But it is the latter, not the former, in which physicians are schooled. And there is very little social science in medical education where one must address the complexities and subtleties of, say, emotion, or ritual, or culture.
If you detect shades of Deepak Chopra in there, you are correct, all with a dollop of utter contempt for Newtonian physics, which, I will remind you, are still accurate enough for most real-world purposes here, where few things we do reach relativistic speeds. Instead, Moerman invokes quarks, quantum theory, and other complexities and contrasts it to the “simpler” sciences that physicians apparently learn. One can almost feel the contempt for us poor, deluded physicians. Perhaps if I had known a bit about Professor Moerman, my jaw ouldn’t have dropped so far when I read this in the editorial accompanying the NEJM study:
What do we learn from this study? The authors conclude that the patient reports were “unreliable,” since they reported improvement when there was none — that is, the subjective experiences were simply wrong because they ignored the objective facts as measured by FEV1. But is this the right interpretation? It is the subjective symptoms that brought these patients to medical care in the first place. They came because they were wheezing and felt suffocated, not because they had a reduced FEV1. The fact that they felt improved even when their FEV1 had not increased begs the question, What is the more important outcome in medicine: the objective or the subjective, the doctor’s or the patient’s perception? This distinction is important, since it should direct us as to when patient-centered versus doctor-directed care should take place.
Apparently Moerman thinks that patient-centered care means inducing a patient through placebo responses to think that he feels better when in actuality the disease-impaired function of his organ (in this case, the lungs) puts him at risk for serious complications. He then goes on to write:
For subjective and functional conditions — for example, migraine, schizophrenia, back pain, depression, asthma, post-traumatic stress disorder, neurologic disorders such as Parkinson’s disease, inflammatory bowel disease and many other autoimmune disorders, any condition defined by symptoms, and anything idiopathic — a patient-centered approach requires that patient-preferred outcomes trump the judgment of the physician. Under these conditions, inert pills can be as useful as “real” ones; two inert pills can work better than one; colorful inert pills can work better than plain ones; and injections can work better than pills.
I find it hard not to notice that Moerman has cast a very wide net; virtually any condition outside of trauma could fit into his definition. I can’t help but think that, if I, for instance, had asthma and the severity of my symptoms didn’t correlate well with my objectively measured lung function as estimated by FEV1, then I would want my lung function tuned up. And if I didn’t want my lung function to be improved, I would hope that my doctor would be able to educate me as to why it is important to make my lungs function better, even though I feel OK. Moerman would seem to advocate telling me, “Oh, no, Dr. Gorski, don’t worry about those blue lips you have. That’s just an ‘objective’ finding. You feel OK, and, since I practice ‘patient-centered’ care, which teaches, among other things, that symptoms are the most important thing and the reason why you come to a doctor in the first place, your feeling better is all that matters!”
I’ll give you another example. Consider an epidural hematoma. If you crack your head hard enough, it can sheer or damage one of the epidural arteries. The typical clinical course is that the patient will be knocked unconscious due to head trauma. Later, he will regain consciousness and experience what is known in the biz as a “lucid interval” that can last several hours. What’s happening during that “lucid interval” is that the blood is still accumulating, but the hematoma hasn’t reached a large enough size yet to cause damage, but when it does the patient deteriorates rapidly. Frequently, one of those “objective findings” is a CT scan that shows a little epidural hematoma, which may or may not blossom into a life threatening epidural hematoma that can squash the brain against the inside of the skull. That’s an “objective” finding. Even though the patient feels well; that hematoma could expand and kill him in a few hours.
No doubt Professor Moerman or Ted Kaptchuk would claim that these are ridiculous and unfair examples. No doubt they would say that this is not what they’re talking about, and that’s probably true. I’ll even concede that the example of the epidural hematoma example was a bit over the top, but that was intentional.
However, whether they realize it or not, by elevating the subjective beyond the objective, and then offering placebo medicine for the subjective, these are exactly the sort of arguments they are making, when you strip them to their essence. No doubt Moerman or Kaptchuk would like to think that they would never, ever use such an approach for diseases with such potentially bad outcomes, but where do they draw the line? When, exactly, do we decide that subjective improvement is more important than objective improvement and by what criteria?Moerman makes a great show of saying, “First, do no harm”:
Do we need to control for all meaning in order to show that a treatment is specifically effective? Maybe it is sufficient simply to show that a treatment yields significant improvement for the patients, has reasonable cost, and has no negative effects over the short or long term. This is, after all, the first tenet of medicine: “Do no harm.”
Clearly implicit in Moerman’s statement is the assumption that not intervening in the abnormal physiology of some diseases (for instance, asthma) doesn’t do harm. He’s wrong. Sometimes doing nothing is harmful, as it allows the disease to continue unchecked, possibly resulting in permanent end organ damage or even the death of the patient, and placebo medicine does nothing to prevent that.
Let’s return to asthma, since that is the disease that this study examined. Even if a person with asthma seems to feel fine with a lowered FEV1, there is a price to be paid for leaving asthma untreated, which, let’s face it, is what placebo medicine is, leaving the functional disorder untreated. For instance, there is evidence that early treatment after the diagnosis is made can prevent the airway remodeling that occurs in chronic asthma, in which airway constriction and inflammation lead to further narrowing of the airway and further functional decline. Moreover, if a case of asthma’s severe enough, a patient could be walking on the proverbial tightrope, where all it would take is a small insult to push him over into a life-threatening asthma exacerbation or pneumonia, whereas if lung function in an asthmatic is tuned up as well as it can be, I’ll have a lot farther to deteriorate to reach that dangerous point. Let’s also not forget: Asthma can and does kill, some 250,000 deaths per year worldwide. Choosing alternative medicine over effective asthma treatment because placebo responses lead to feeling better without altering the underlying illness, could very well lead to preventable asthma deaths.
In the end, I’m a bit torn about this study. On the one hand, it irritates me to no end how it is being sold to the public as evidence of “powerful” placebo effects and as evidence that we physicians should be doing more placebo medicine. On the other hand, the fact that CAM advocates are reduced to spinning studies like this the way they are is pretty darned conclusive evidence that they now know that, from the standpoint of therapy, the vast majority of CAM modalities do nothing and are in fact placebo medicine. The problem is, in some diseases, such as asthma, placebos run the risk of allowing serious harm from lack of effective intervention that actually alters the course of disease. If the therapeutic relationship is so damaged in the U.S. that the beneficial effects of provider-patient interactions are not being realized, whether you want to refer to these effects at the “placebo response” or something else, the answer is to fix medicine to make it easier and more rewarding for physicians to spend that time with patients. The answer is not to embrace magical thinking like that behind acupuncture, homeopathy, and huge swaths of CAM. To argue otherwise is a false dichotomy.
![]()
![]()
![]() <!--<!--
<!--<!--![]()
![]()
![]()
![]()
Don’t Let IPv4 Exhaustion Sneak Up on You
A few month ago, IANA exhausted its unallocated IPv4 address pool when it gave the last /8‘s to regional registries around the world. That news got a fair amount of buzz. Last month, some of the biggest sites in the world participated in World IPv6 Day to a little fanfare as well. Following those larger flows of attention have been the inevitable ebbs as people go back to “business as usual.” As long as ARIN has space available (currently 4.93 /8s in aggregate), no one is losing sleep, but as that number continues decreasing, and the forced transition to incorporate IPv6 will creep closer and closer.
On July 14, I was honored to speak at IPv6 2011: The Time is Now! about how technology is speeding up IPv4 exhaustion and what the transition to IPv6 will mean for content providers. Since the session afforded me a great opportunity to share a high level overview of how I see the IPv4-to-IPv6 transition (along with how SoftLayer has prepared), it might be interesting to the folks out there in the blogosphere:
As time goes by, these kinds of discussions are going to get less theoretical and more practical. The problem with IPv4 is that the entire world is about to run out of free space. The answer IPv6 provides is an allocation pool that is not in danger of exhaustion. The transition from IPv4 to IPv6 isn’t as much “glamorous” as it is “necessary,” and while the squeeze on IPv4 space may not affect you immediately, you need to be prepared for the inevitability that it will.
Technology Partner Spotlight: Papertrail
Welcome to the next installment in our blog series highlighting the companies in SoftLayer’s new Technology Partners Marketplace. These Partners have built their businesses on the SoftLayer Platform, and we’re excited for them to tell their stories. New Partners will be added to the Marketplace each month, so stay tuned for many more come.
- Paul Ford, SoftLayer VP of Community Development
Scroll down to read the guest blog from Troy Davis of Papertrail, a SoftLayer Tech Marketplace Partner that helps customers detect, resolve and avoid infrastructure problems using log messages. To learn more about Papertrail, visit http://papertrailapp.com/.
Receive DB Slow Query Logs in Your Inbox
Want to wake up to important database and syslog messages with your bagel and coffee? Here’s how. It’s free and takes about 5 minutes.
Most of us run a database somewhere on our SoftLayer servers. Whether it’s MySQL, PostgreSQL, SQL Server, or another relational or NoSQL sibling, a responsive data store is critical to happy users. That’s why databases send slow queries to a log file. It’s much better than no logging at all, but as an engineer, I’d wanted more. I wanted to:
- View all my query logs in one place, without SSHing to each server for tail and grep. My workload shouldn’t scale linearly as I add systems
- Share log visibility with employees who don’t have server access or command-line knowledge (and email links to specific log messages to my developers and DBAs)
- Receive log messages in my inbox – or send them to my team or monitoring service – when I know they need attention
- Examine logs for related HTTP requests, daemon output, API invocations, and other parts of our stack — I can troubleshoot faster with start-to-finish logs on a single screen.
That’s where Papertrail was born. We built Papertrail to make log aggregation and log management effortless and usable. It’s the hosted log management service that we wanted as developers, systems engineers and tech entrepreneurs.
We know the hesitation you might have when approaching this kind of service, so our goal was to enable users to have Papertrail deliver those SQL slow query logs – or any other logs – to your inbox every morning for free:
1. Register a Papertrail log Repository
Hit https://papertrailapp.com/plans and sign up. You’ll land on a welcome page. From there, click the “Add System” link, and on the form shown, type the IP of your DB server and its name (like “db1″).
Papertrail will display a remote syslog destination for your logs and easy instructions for sending app log files and syslog. The steps below are customized for MySQL’s slow query log.
2. Send MySQL logs
Install a log sender. To install a tiny standalone binary that sends log file contents to Papertrail as they occur without any other system-wide configuration changes, with Ruby you can run the “gem” binary: sudo gem install remote_syslog
Next, locate your MySQL or other database slow query log file. Usually these are in the directory /var/mysql/log/ or /var/log/mysql/, usually with a filename containing “slow”. An example slow query log path is: /var/log/mysql/mysql-slow.log
If you don’t see one, try running “locate mysql | grep slow.log” (or to configure a slow query log, head here).
Next, tell remote_syslog the path to that file. Edit /etc/log_files.yml and add a single line:
files: [/var/log/mysql/mysql-slow.log]
Use the path to your slow query log (Example). Finally, run remote_syslog:
sudo remote_syslog
3. Set up Nightly Email
Now that you’ve completed those first two steps, you’re configured to send those slow query logs to Papertrail as soon as they happen. Hit Papertrail’s events viewer to watch them roll in. Because only slow queries are being logged, you may not see any events immediately.
To receive these messages in email, search Papertrail’s events viewer for ‘mysql’. Then click “Save Search” and give this search a name (like “MySQL slow queries”). Click the Dashboard link and you’ll see that search as a new choice. Click the Edit link next to it, and you’ll be prompted for the email address(es) which should receive these in email every night.
That’s it. Congrats! If you were hoping for more steps, I’d recommend that you get yourself a Doppelbock or porter as Step 4.
You have the ability to give co-workers access to these logs in Papertrail, and because Papertrail doesn’t charge a per-system fee, you can add other systems at will. With your SQL logs done, it only takes a few more minutes to aggregate Web server request logs and OS syslog results from your dedicated and CloudLayer systems (try “Add System” or “Quick Start”).
Enjoy!
- Troy Davis, Papertrail
PHIL’s DC: A Tour of the Facility
In the second episode of my self-made documentary series about the birth of a revolution in hosting, I explained how Lance and I mutually decided that a better course of action would be to build a data center for the future’s future, and I sketched out the basics of effective data centering. Lance sent the keys to the new non-traditional facility, and I jumped at the chance to give a tour of the amazing digs.
Because I wanted to make sure to document as much of the process as I could for this documentary film (I’m coming for you, The Social Network), you’re experiencing the tour as I explore the space for the first time, so I hope you find it as magical as I did. Note: I took the liberty of acquiring suitable transportation to give you the most professional “tour” experience.
{kind=link}
You’ll note that the facility features several important characteristics of the best data center environments:
- Heightened Exterior Security
- Data Center Operations Area
- Weather Tracking Station
- Tech Support Center
- CEO Suite
- Redundant Bandwidth Providers
- Multi-phase Power
- Power Generator
- Built-in Cooling
- Crash Cart Station
- Vaulted Ceilings (for warm air circulation)
Now that I’ve got the lay of the land, it’s just a matter of drawing up some plans for server racks, plugging in some servers and getting some customers to experience the newest wave of hosting innovation!
-PHIL
Parliament receive copies of spiritual enlightment book – GhanaWeb
Parliament receive copies of spiritual enlightment book GhanaWeb Accra, July 22, GNA – Parliament on Friday received 250 copies of spiritual enlightenment book known as the Zahar, from students of the Kabbalah Centre, London, United Kingdom. Mrs. Zeta Annan, who made the presentation, said the Zahra is a historical ... |
KC group finds enlightenment with the Dalai Lama – Kansas City Star
 Kansas City Star | KC group finds enlightenment with the Dalai Lama Kansas City Star Among the enthusiastic fans are eight road trippers (and one reporter) ranging from 24 to 72, who have traveled from Kansas City to Fayetteville to soak up enlightenment from the 76-year-old spiritual leader with the shaved head, cherubic demeanor and ... |
Author explores path to personal enlightenment – Waterloo Cedar Falls Courier
Author explores path to personal enlightenment Waterloo Cedar Falls Courier In "The Soul Solution," Parker emphasizes the reader's spiritual journey into healing, personal transformation and enlightenment. He also offers spiritual wisdom and self-guided practices he believes will lead to inner transformations that lead to ... |
‘Dexter’ Season 6 Trailer: Dexter Searches For Faith – Screen Rant
 Screen Rant | 'Dexter' Season 6 Trailer: Dexter Searches For Faith Screen Rant As teased in last week's promo, Dexter may be on the path of spiritual enlightenment this season, perhaps transitioning the concept of his dark passenger from insatiable need to doing good work for the man upstairs. Hall suggests that the character's ... |
A bookshelf the size of the world – Boston Globe
Boston Globe | A bookshelf the size of the world Boston Globe .The Enlightenment uses this idea of the republic of letters, meaning there would be a kind of literary or spiritual world with no police and no boundaries and no linguistic or disciplinary borders, and that this world would be open to everyone, ... |
San Francisco circumcision ban vote may be derailed by new bill – Kansas City Star
San Francisco circumcision ban vote may be derailed by new bill Kansas City Star "To enact an outright ban on an expression of personal, medical and religious freedom is an affront to all who value liberty," said Assemblyman Mike Gatto, a Los Angeles Democrat who proposed AB 768. San Francisco's first-of-its-kind initiative has ... |